Statistics on Oral Health Among Pregnant Women
Reader-supported. We may earn a commission from links on this page. Advertising disclosure.
In this article
Maintaining good oral health during pregnancy is often overlooked, yet it is a crucial component of prenatal care. Hormonal shifts and dietary changes can increase the risk of gum inflammation and dental caries, making pregnant individuals more vulnerable to oral health problems that can persist if left unaddressed.
Pregnancy is also a “teachable moment,” during which expectant mothers may be more receptive to health advice. Despite growing awareness of the safety and importance of dental care, many pregnant women still face barriers to routine treatment.
Looking at the statistics, trends, and challenges around pregnancy and oral health helps clarify the scope of the issue and where care can improve.
Key Statistics at a Glance
- 60% to 75% of pregnant women are affected by gingivitis at some point during pregnancy.
- Fewer than 50% of pregnant women in the United States receive a dental cleaning or checkup while pregnant.
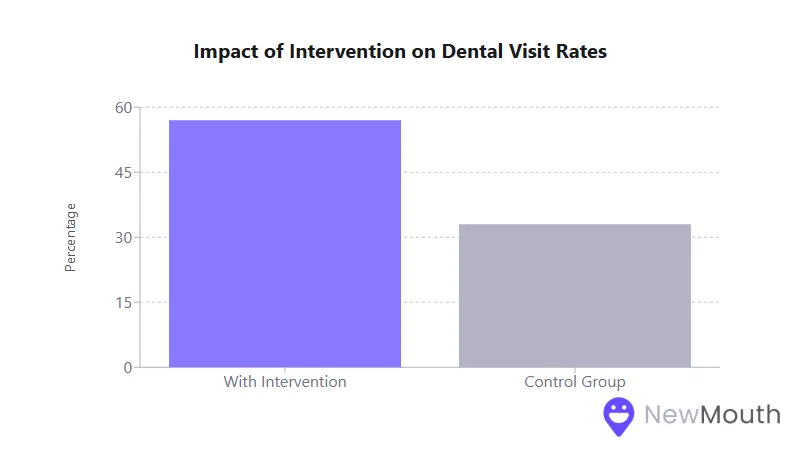
- In one low-income intervention trial, a 57% dental visit rate was achieved when proactive education and referrals were offered (compared to 33% in the control group).
- Approximately 30 to 40% of pregnant individuals have some form of periodontal disease, a condition linked (though not conclusively causative) to higher rates of adverse birth outcomes.
The Importance of Understanding Trimester-Specific Changes
During pregnancy, physiological and hormonal shifts can significantly impact oral health. Recognizing how these changes unfold by trimester helps clinicians and patients tailor their preventive strategies:
- Increased Gingivitis Risk
- Gingivitis peaks in the third trimester, largely due to higher estrogen and progesterone levels exacerbating gum inflammation.
- Roughly 60% to 75% of pregnant women experience gum bleeding, swelling, or tenderness at some stage.
- “Pregnancy Tumors” (Pyogenic Granulomas)
- Around 5% of pregnancies involve benign overgrowths on the gums, typically arising after the first trimester.
- These growths usually regress postpartum but can cause discomfort or interfere with oral hygiene if left unchecked.
- Enamel Erosion and Dental Caries
- Frequent nausea and vomiting in early pregnancy expose teeth to additional acids.
- Dietary cravings for sugary or acidic foods may increase cavity risk, especially if oral hygiene lapses.
Understanding these trimester-specific developments underscores why timely dental visits, especially early in pregnancy, can prevent minor problems from escalating.
Safety of Dental Treatment During Pregnancy
It is well-established that dental care is safe throughout all stages of pregnancy. Both preventive and restorative procedures pose minimal risk when performed correctly:
- Routine Treatments and X-Rays
- Cleanings, fillings, root canals, and extractions are considered safe at any point.
- Dental X-rays are acceptable with proper shielding, and local anesthetics, including those containing epinephrine, are also safe when used judiciously.
- Second Trimester Comfort
- The second trimester (14 to 20 weeks) is often recommended for non-urgent procedures since it is typically the most comfortable period for the patient.
- However, urgent dental issues (such as significant decay or infection) should be addressed promptly in any trimester.
Dentists and obstetric providers alike emphasize that leaving dental problems untreated during pregnancy can be more harmful than receiving appropriate care. By coordinating with prenatal providers, dentists can deliver necessary treatments without undue delay and help prevent more severe complications later.
Prevalence and Severity of Gingivitis in Pregnancy
Gingivitis remains the most frequent oral health concern among pregnant individuals:
- Affects an estimated 60% to 75% of pregnant women in the United States.
- Often worsens in those with pre-existing gum inflammation, peaking in the third trimester.
- Typically presents as redness, swelling, and bleeding, but can progress to deeper periodontal disease if neglected.
Although pregnancy gingivitis is generally mild and reversible with proper oral hygiene and professional care, the high prevalence underscores the importance of early detection and regular dental checkups.
Disparities in Access to Dental Care
Despite the recognized importance of oral health during pregnancy, less than half of pregnant women nationwide receive any dental care:
- 46% of U.S. pregnant women undergo dental prophylaxis (cleaning), according to some national reports.
- In certain low-income populations, historical rates of dental visits during pregnancy can be as low as 23% to 35%.
- States that have expanded Medicaid coverage to include dental benefits for pregnant women have noted modest increases in dental visits (e.g., from 30% to nearly 38% in one program).
Barriers to care include cost, limited insurance coverage, misconceptions about safety, and a lack of prenatal providers systematically referring women for dental services. Expanding Medicaid dental benefits and integrating dental screenings into prenatal care are among the strategies states use to improve access.
Effectiveness of Prevention Programs
Prevention-focused interventions have demonstrated success in improving maternal and child oral health outcomes:
- Increased Dental Visits
- A nurse-led referral program raised the rate of dental visits from 33% to 57% among low-income pregnant women.
- Interventions where midwives provided oral health education and referrals achieved attendance of 87.2% in the treatment group vs. 20.2% in usual care.
- Reducing Childhood Caries
- Mothers who receive comprehensive dental care and counseling during pregnancy reduce their children’s risk of early childhood caries by up to 82% (measured at age two).
- Fluoride treatments, professional cleanings, and improved prenatal nutrition contribute to fewer oral bacteria transmitted to infants.
These programs typically combine education, screening, and referrals at prenatal visits, showing how a proactive approach can break the cycle of missed care and subsequent dental disease.
Completing Dental Treatments During Pregnancy
Even when pregnant women are referred for treatment, completion rates can remain a challenge:
- In one state program, only 43% of women with a dental referral actually attended a dentist appointment.
- Common reasons for failing to complete treatment include scheduling difficulties, fear or misconceptions, and the nearing of delivery.
- Models with strong care coordination and direct scheduling have demonstrated completion rates near 90%, highlighting the potential for improvement when logistical barriers are removed.
Because many pregnant individuals lose or change insurance coverage soon after giving birth, it is crucial to ensure they receive definitive treatment before delivery. Streamlined referrals, sometimes even scheduling the dental appointment while the patient is in the prenatal clinic, can boost follow-through.
Provider Awareness and Collaborative Care
Awareness of pregnancy oral health guidelines has grown, but knowledge gaps persist:
- Among General Dentists
- About 94% say they perform routine exams for pregnant patients.
- Around 90% believe restorative procedures are safe, though about half feel inadequately trained by their dental schools on the specifics of pregnant-patient care.
- Among Obstetric Providers
- Roughly 57% of prenatal care clinicians are aware of national guidelines on pregnancy oral health.
- Not all obstetricians or midwives routinely ask about dental concerns or refer patients, often due to limited training or uncertainty about the dentist’s role.
Continued professional education on both sides is critical. Dentists must be comfortable providing comprehensive care to pregnant patients, and obstetric providers should incorporate oral health screenings into prenatal visits. Clear guidelines help foster collaborative care and dispel myths about treatment risks.
Oral Health Risk Factors and Pregnancy Outcomes
Research has consistently examined a possible link between periodontal disease and adverse birth outcomes:
- Periodontal Disease Prevalence
- Affects 30 to 40% of pregnant individuals.
- Characterized by deeper gum infection involving bone loss.
- Potential Impact on Prematurity
- Observational studies have found higher rates of preterm birth or low birth weight among women with severe periodontal disease.
- However, randomized controlled trials providing periodontal therapy in mid-pregnancy have shown mixed or no effect on reducing preterm delivery, suggesting the relationship may be correlational rather than strictly causal.
Poor oral hygiene and high bacterial counts can also increase a child’s risk of early childhood caries after birth. Although definitive proof that treating gum disease alone prevents adverse outcomes remains elusive, experts advocate addressing oral health early, ideally before or in the first half of pregnancy, to minimize potential risks.
Educational Programs to Improve Pregnancy Oral Health
Structured oral health education has been shown to modify dental habits and attitudes during pregnancy:
- Longer Brushing Durations
- One 2022 trial reported that the proportion of pregnant women brushing for at least two minutes rose from ~52% to 76% after an educational intervention.
- Ongoing Behavior Change
- Women who received comprehensive counseling demonstrated better oral hygiene practices postpartum than those who received only written materials.
These programs typically focus on:
- Explaining why pregnancy raises susceptibility to gum inflammation
- Demonstrating proper brushing and flossing
- Offering nutrition guidance to reduce sugary snacking
- Stressing the safety of dental treatments while pregnant
When integrated into prenatal classes or clinical visits, these sessions improve both the mother’s oral health and the baby’s future oral health.
Insurance Coverage Trends for Pregnant Patients
Dental coverage for pregnant individuals in the United States has expanded noticeably over the last two decades:
- Medicaid Expansions
- All 50 states now provide at least emergency-only dental coverage to pregnant Medicaid enrollees.
- 39 states and Washington, D.C. extend more comprehensive coverage to this group, a major improvement from years past.
- Postpartum Extensions
- Traditionally, Medicaid pregnancy dental benefits end around 60 days postpartum.
- Many states now offer a 12-month postpartum extension, giving mothers more time to complete any pending treatments.
Private insurers often include prenatal dental exams in their maternity benefits, though specifics vary by plan. As coverage improves, the hope is that more pregnant individuals will take advantage of preventive services and reduce their reliance on emergency care for avoidable oral issues.
Emergency Dental Care Utilization
When preventive access is limited, pregnant women with severe toothaches or infections may seek urgent treatment in hospital emergency departments:
- A large share of dental-related ED visits in the U.S. involves populations also served by Medicaid, suggesting that limited coverage for routine care often leads to more costly crisis care.
- Studies show that 42% of dental-related ED visits are covered by Medicaid, underscoring how socioeconomically vulnerable groups, including pregnant individuals, may use the ED as a last resort.
- Over 2 million dental-related ED visits occurred nationwide in a recent year, many for issues that would have been better managed and at a lower cost by a dentist in an outpatient setting.
Experts encourage pregnant individuals to treat urgent oral issues promptly rather than waiting until after delivery. Avoiding or delaying care can exacerbate infections, posing a far greater risk to both mother and fetus.
Long-Term Impact of Pregnancy-Related Oral Health Issues
Oral health challenges that arise or worsen during pregnancy can have lasting consequences:
- Progression of Disease
- Untreated pregnancy gingivitis can advance to chronic periodontitis, leading to bone loss and possible tooth loss over time.
- Enamel damage or cavities incurred from frequent vomiting or dietary changes do not simply resolve postpartum; they require intervention.
- Effects on Infant Oral Health
- High bacterial levels in the mother’s mouth are easily transmitted to the newborn through saliva (e.g., sharing utensils), increasing the child’s cavity risk.
- By improving prenatal oral health, mothers reduce the likelihood of early childhood caries in their offspring.
Although certain pregnancy-specific conditions (like “pregnancy tumors”) often subside after childbirth, the structural damage caused by long-standing gum inflammation or decay can persist unless properly treated.
Oral Health and Birth Outcomes (Preterm Birth, Low Birth Weight)
While the evidence of direct causation is inconclusive, ongoing studies continue to explore links between severe periodontal disease and adverse birth outcomes:
- Observational Data
- Some studies indicate that maternal gum disease may double the odds of delivering prematurely or at a low birth weight.
- Bacterial pathogens and inflammatory markers from the mouth can potentially travel to the uterine environment.
- Randomized Trials
- Large interventional trials treating periodontal disease in mid-pregnancy have not clearly demonstrated a reduced risk of preterm birth.
- This suggests poor oral health is more likely a correlate of wider health disparities that also predispose to unfavorable birth outcomes.
Despite these nuances, most health organizations promote oral care as part of comprehensive prenatal services. Improving oral health is viewed as one more way to help minimize risk factors that could contribute to preterm delivery or fetal growth concerns.
Partner Involvement in Oral Health During Pregnancy
Research indicates that involving partners in oral health education may significantly enhance outcomes for pregnant individuals:
- Family-Centered Approach
- When pregnant women and their partners jointly receive oral health counseling, intervention groups often demonstrate lower plaque levels and gum inflammation, sustained even after childbirth.
- Partners can encourage consistent brushing, flossing, dental appointments, and can reinforce healthier dietary choices.
- Long-Term Maintenance
- Such programs also help maintain better oral hygiene habits well into the postpartum period.
- Equipping both parents-to-be with the knowledge and motivation to reduce sugar intake and practice proper oral hygiene can protect the infant’s oral health by limiting bacterial transmission.
Including partners in prenatal dental discussions or scheduling couple-based oral health sessions can amplify the benefits of educational and preventive measures.
Post-Pregnancy Dental Care Patterns
Dental utilization patterns often shift after childbirth:
- Drop in Immediate Postpartum
- Only about 15% of women may seek dental care in the first six months postpartum due to competing demands of newborn care and potential insurance changes.
- For many, routine self-care takes a back seat during this intense recovery phase.
- Gradual Rebound
- Around 75% of women in some studies reported a dental visit by six months postpartum, which is higher than during pregnancy.
- Extended Medicaid coverage to 12 months postpartum, now adopted by numerous states, is expected to improve continuity of care by reducing insurance disruptions shortly after delivery.
Maintaining a regular dental schedule during the postpartum period is vital. Addressing any unmet needs from pregnancy can prevent further complications and set a positive health precedent for the entire family.
Final Summary
Many pregnant individuals face heightened oral health challenges, including an increased susceptibility to gingivitis, dental caries, and periodontal disease. Although scientific consensus about the direct impact of gum disease on adverse birth outcomes remains mixed, experts agree that prompt dental treatment benefits overall well-being.
Statistics reveal persistent barriers in accessing consistent prenatal dental care. By ensuring collaborative care among obstetric providers, dentists, and families, oral health can be addressed proactively as part of routine prenatal services.
Continued efforts to educate healthcare professionals, integrate dental referrals in prenatal clinics, and offer comprehensive insurance benefits will help close the gaps. Policies that extend dental coverage beyond pregnancy, along with well-designed public health programs, support mothers during the often-overlooked postpartum phase.
Sources
- American College of Obstetricians and Gynecologists. “Oral Health Care During Pregnancy and Through the Lifespan.” ACOG Committee Opinion No. 569, 2013; reaffirmed 2025.
- American Dental Association (ADA) – https://www.ada.org/resources/ada-library/oral-health-topics/pregnancy
- American Public Health Association (APHA) – https://www.apha.org/policies-and-advocacy/public-health-policy-statements/policy-database/2021/01/12/improving-access-to-dental-care-for-pregnant-women
- Centers for Disease Control and Prevention (CDC) – https://www.cdc.gov/oral-health/data-research/facts-stats/fast-facts-pregnancy-and-oral-health.html
- Comprehensive pregnancy dental benefits improved dental coverage among Medicaid-enrolled pregnant women in Virginia – https://www.ncbi.nlm.nih.gov/pmc/articles/PMC9530928
- Effectiveness of a family-centered behavioral and educational counselling approach to improve periodontal health of pregnant women: a randomized controlled trial – https://www.ncbi.nlm.nih.gov/pmc/articles/PMC7568358
- Emergency Department Visits Involving Dental Conditions, 2018 – https://hcup-us.ahrq.gov/reports/statbriefs/sb280-Dental-ED-Visits-2018.pdf
- Oral Health During Pregnancy, American Academy of Family Physicians (AAFP) – https://www.aafp.org/pubs/afp/issues/2008/0415/p1139.html
- Promoting Oral Health Behavior During Pregnancy: A Randomized Controlled Trial – https://www.ncbi.nlm.nih.gov/pmc/articles/PMC10422136
- A Successful Dental Care Referral Program for Low-Income Pregnant Women in New York – https://www.ncbi.nlm.nih.gov/pmc/articles/PMC8656616
- State Medicaid Coverage of Dental Services for General Adult and Pregnant Populations – State Medicaid Coverage of Dental Services for General Adult and Pregnant Populations
- Utilization of dental services among low and middle income pregnant, post-partum and six-month post-partum women – https://pubmed.ncbi.nlm.nih.gov/32312257

Web content writer specializing in making dental research accessible to diverse audiences.
Related Articles

Best Foods for Healthy Teeth and Gums
What you eat plays a crucial role in maintaining a healthy mouth, and below we cover the best foods to incorporate into...

Best Natural Remedies for Treating Gum Disease
Having a good oral care routine is a great way to prevent gum disease and build the foundation for healthy gums. But the...
How Does Dental Anxiety Affect Your Oral Health?
Dental anxiety (everything from mild nervousness to severe dental phobia) affects a significant portion of the populatio...
Dental Care Spending: Statistics and Trends
Dental expenditures in the United States have steadily risen over the past decade, reflecting shifts in procedure costs,...