What Is the Effect of Socioeconomic Status on Oral Health?
Reader-supported. We may earn a commission from links on this page. Advertising disclosure.
In this article
Socioeconomic status (SES) is a major predictor of who can access quality dental care and who struggles with preventable oral health issues. While overall oral health outcomes in the U.S. have shown modest improvements over time, wide disparities persist among lower-income groups, those with less education, and the uninsured.
Here we explore statistics detailing how socioeconomic status impacts oral health outcomes, access to care, treatment completion, and the effectiveness of public programs. By examining these data points, we gain insight into the financial, geographic, and systemic barriers that perpetuate inequalities in dental health.
Overview of the Topic
Oral health plays a key role in overall well-being; poor dental health often correlates with chronic conditions such as diabetes and cardiovascular disease. Over the past decade, researchers have documented significant gaps in who can consistently access preventive services and restorative treatment.
Key factors include household income, educational level, insurance status, and geographic location (e.g., rural versus urban communities). Public programs like Medicaid, the Children’s Health Insurance Program (CHIP), and school-based initiatives have helped reduce cavities among children, yet many adults remain without coverage or face high out-of-pocket costs.
Addressing oral health disparities is part of a broader public health imperative to reduce inequalities in the U.S. This article compiles the most recent and reputable data to illustrate trends in oral health disparities, providing insight into challenges and spotlighting interventions that have proven effective in underserved communities.
Noteworthy Statistics
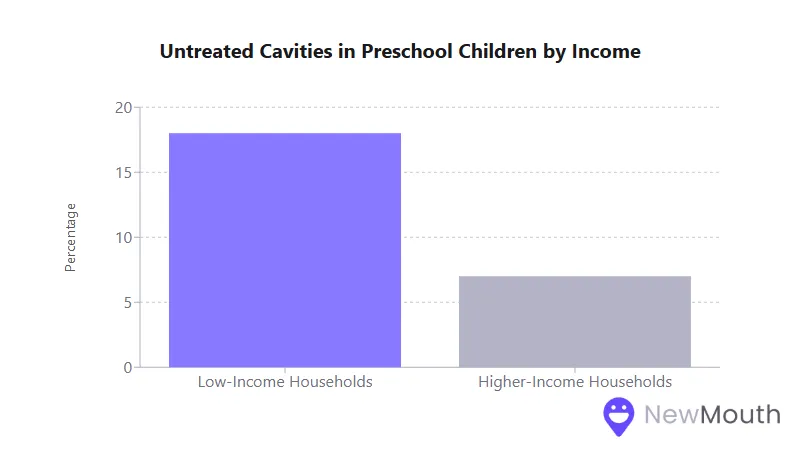
- Untreated cavities are nearly three times more common in preschool-age children from low-income households compared to children in higher-income families.
- Over 68 million adults in the United States lack dental insurance, a figure disproportionately affecting low-income individuals and racial or ethnic minorities.
- Rural communities, which constitute large low-income populations, experience 8 to 10% less access to dental services compared to metropolitan areas.
- States that expanded Medicaid to include comprehensive adult dental benefits saw a 14% reduction in non-traumatic dental emergency room visits, while states without such coverage saw increases.
Correlation with Income Levels
Income level is one of the strongest predictors of oral health disparities. Understanding how financial resources affect care access and disease prevalence is key to designing effective interventions.
- Preventive Visits: In multiple national surveys, only about 28% of individuals living in poverty had a dental visit in the past year, compared to 55% of those with higher incomes.
- Disease Burden: Preschool children in low-income households show an untreated cavities rate of around 18%, nearly three times that of higher-income peers (~7%).
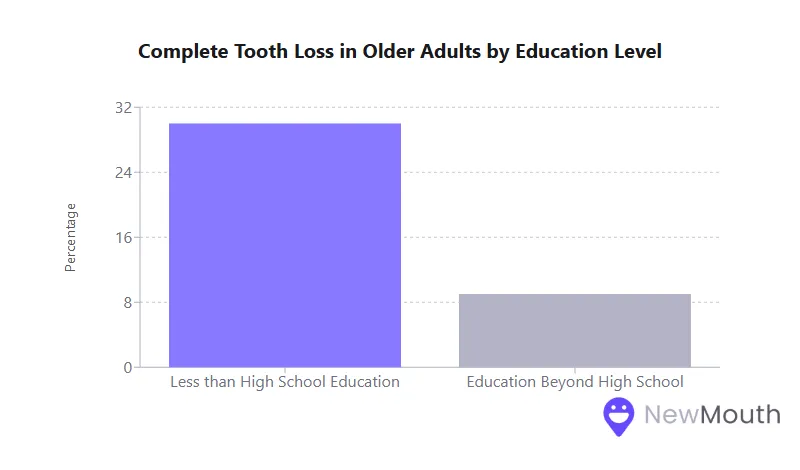
- Tooth Loss: Among older adults, complete tooth loss (edentulism) is more than twice as common in low-income households (around 30%) versus wealthier groups (about 12%).
Because oral health problems tend to compound over time, lower-income individuals face a lifetime of higher disease risk, culminating in tooth loss and a higher incidence of emergency dental visits.
Impact of Education on Oral Health Outcomes
Education level often parallels income, but it also independently shapes oral health behaviors, awareness, and the likelihood of seeking professional care.
- Higher Risk of Tooth Loss: Among older adults with less than a high school education, rates of complete tooth loss can exceed 30%, compared to about 9% for those who pursued education beyond high school.
- Parent Education and Child Health: Research shows that caregivers with a high school diploma are nearly 1.8 times more likely to obtain routine dental care, and their children are about 6 times more likely to receive regular checkups than those whose parents did not graduate.
- Preventive Behavior: Individuals with higher education tend to be more proactive in scheduling preventive services, including annual exams and routine cleanings, helping limit severe gum disease and decay.
Boosting oral health literacy through community education programs can significantly improve outcomes, especially when coupled with accessible services.
Patterns of Insurance Coverage
Insurance coverage has a direct bearing on the affordability and utilization of dental care. Examining patterns in who has coverage and what type is critical to understanding service gaps.
- Lack of Coverage: An estimated 68.5 million adults in the U.S. have no dental insurance. Uninsured rates are significantly higher in low-income groups, where fewer than 1 in 5 low-income adults hold a private dental plan.
- Medicaid/CHIP for Children: Most states provide dental benefits for children through Medicaid and CHIP, improving access for lower-income minors. Indeed, about half of children on Medicaid/CHIP receive at least one dental service yearly, though disparities by location and ethnicity remain.
- Patchwork Adult Benefits: Adult dental coverage in Medicaid is optional for states. As of recent surveys, around 17 states offer comprehensive adult benefits, while others limit coverage to extractions or emergency-only care. In states lacking broader benefits, low-income adults often avoid or delay dental procedures until pain becomes severe.
These insurance patterns highlight why many in lower socioeconomic tiers face an uphill battle in affording treatment, especially restorative or specialized services.
Treatment Completion Rates
Receiving a treatment plan does not guarantee completion, especially when social and financial barriers arise.
- Orthodontic Treatment: In one rural Appalachian sample, only 34% of patients receiving braces through Medicaid or CHIP completed treatment, compared to 74% among self-paying patients.
- Interrupted Care: Cost hurdles and transportation challenges often lead lower-income individuals to abandon multi-visit treatments. Many opt for extractions in emergency settings rather than restorative care that involves multiple appointments and higher expenses.
- Follow-Up Gaps: Even when aware of treatment needs, caregivers in low-SES households report struggles with scheduling, missing work, and affording co-pays, leading to incomplete procedures or reliance on temporary fixes.
Efforts such as case-management services, sliding-scale fees, and mobile clinics can improve follow-through on dental treatments.
Access to Preventive Programs
Preventive care, especially for children, is widely considered the most cost-effective strategy to reduce long-term disease. Yet, low-SES communities consistently receive fewer preventive services.
- Preventive Visits: Only about one-quarter of low-income working-age adults reported any dental visit in the past year, compared to over half of those with higher incomes.
- Sealants and Fluoride: School-based sealant programs prevent roughly 80% of cavities in treated back teeth, and community water fluoridation reduces tooth decay by about 25% overall. However, low-income and minority children still have lower sealant rates than their higher-income counterparts.
- Underutilization: Factors like provider shortages, language barriers, and low health literacy all compound to reduce the use of regular checkups, fluoride treatments, and sealants in disadvantaged neighborhoods.
When targeted preventive programs, like free school-based sealant initiatives, are available, they have proven highly effective at narrowing disparities for children.
Emergency Care Utilization
Without reliable preventive or restorative care, many low-income and uninsured individuals turn to hospital emergency departments for urgent oral health needs.
- ED Visit Rates: In the poorest communities, dental-related ED visits can exceed 1,000 per 100,000 people, a rate several times higher than in wealthier areas. Young adults and uninsured or Medicaid-insured individuals account for a significant portion of these visits.
- Limited Treatment in EDs: Most emergency rooms can only manage symptoms (pain control, antibiotics), not perform definitive procedures like root canals or fillings. This often leads to recurring pain and higher overall healthcare costs, estimated at nearly $2 billion yearly in ER-related dental visits.
- Medicaid Expansion Impact: States that expanded Medicaid to include adult dental benefits saw a 14% decrease in non-traumatic dental ER visits, confirming that broader coverage steers patients toward dental offices for earlier and more appropriate treatment.
High rates of dental emergencies among low-SES groups underscore how gaps in routine access transform manageable dental issues into costly crises.
Geographic Distribution of Disparities
Location often amplifies socioeconomic challenges, with rural areas and certain regions enduring some of the worst oral health outcomes.
- Rural Disadvantages: Rural residents have about 8 to 10% lower access to dental services than their urban counterparts. About 57 million Americans live in designated Dental Health Professional Shortage Areas, most of them in rural regions.
- Regional Hot Spots: The Appalachian region and the Deep South (e.g., Mississippi Delta) exhibit some of the highest rates of tooth loss and untreated decay. In West Virginia, over one-third of seniors have lost all their teeth, well above the national average.
- Urban Underserved: Inner-city “dental deserts” also exist, where few or no providers accept Medicaid or discounted payments, leaving high-poverty neighborhoods with limited or no local dental resources.
Geographic inequalities highlight the need to incentivize providers to practice in underserved areas and to develop mobile or tele-dentistry programs for hard-to-reach populations.
Correlation with Provider Availability
Even if individuals have insurance, a scarcity of providers willing or able to serve low-SES communities can restrict actual access to care.
- Shortage Areas: Over 57 million Americans live in federally designated shortage areas for dental health professionals, often located in lower-income rural and inner-city regions.
- Medicaid Acceptance: Many dentists limit or refuse Medicaid patients due to lower reimbursement rates, effectively shrinking the provider pool for economically disadvantaged groups.
- Influence on Utilization: Studies consistently show that when new dental clinics open in low-income communities, usage rises accordingly and ER visits for dental issues drop. Conversely, a lack of local providers leads to delayed care and higher emergency utilization.
Efforts to expand mid-level dental providers and improve Medicaid reimbursement rates are ongoing strategies to boost provider participation in underserved settings.
The Impact of Cost Barriers
Cost is consistently the most cited barrier preventing Americans, particularly those with lower incomes, from seeking timely dental care.
- Skipping Care: Surveys show that 1 in 4 low-income adults skips needed dental care each year because they cannot afford it.
- Out-of-Pocket Burden: Unlike general medical care, where only about 11% of costs are paid out of pocket, patients pay around 40% of dental costs themselves. Poorer families also pay 7 times more of their income share on dental care compared to wealthier households.
- Trade-Offs: High prices push many individuals to opt for extractions instead of restorative procedures (such as root canals and crowns), which are significantly more expensive. The result is long-term oral health damage and, ironically, higher costs down the line.
Addressing affordability through expanded coverage, discounted clinics, and flexible financing options is central to reducing disparities in oral health outcomes.
Variations in Quality of Care
SES differences are evident not only in whether people get care but also in the types of services provided and the continuity of that care.
- Restorative vs. Extraction: Adult Medicaid benefits in some states cover extractions for pain relief but not crowns or root canals. Consequently, low-income individuals may lose teeth that wealthier patients can save.
- Safety-Net Systems: Community health centers play a crucial role but often operate with limited resources and high demand, leading to waitlists or shorter appointment times.
- Specialty Access: Comprehensive care often requires specialists like oral surgeons or endodontists, services that low-income and uninsured patients frequently struggle to afford or locate.
Bridging these quality gaps requires integrated care systems, higher reimbursement rates, and robust safety-net funding so that lower-SES patients receive the same range of services as everyone else.
Treatment Delay Patterns
Socioeconomic barriers commonly result in delayed treatment, which exacerbates disease progression and health complications.
- Waiting Until It Hurts: Many uninsured or underinsured individuals avoid dental visits until pain or infection becomes acute. Roughly 18 to 20% of working-age adults report not receiving needed dental care in the last year, a proportion that rises to 33% among low-income groups.
- Progression of Disease: Small cavities, when left untreated, often evolve into major abscesses or gum disease. Delayed care leads to more expensive treatments like root canals or extractions if restoration is no longer viable.
- Cultural Norms: In communities with a historic lack of access, people may not see regular cleanings as necessary. Addressing this pattern requires consistent community-based outreach combined with affordable care options.
When individuals finally seek help after months or years of avoidance, the cost and complexity of treatment can be markedly higher, reinforcing the cycle of poor oral health.
Long-Term Health Outcomes
Oral health disparities have ripple effects on general health and well-being.
- Chronic Disease Connections: Gum disease, twice as prevalent in low-income adults, is closely linked with diabetes, cardiovascular problems, and other inflammatory conditions.
- Nutrition and Quality of Life: Missing teeth can limit food choices, contributing to nutritional deficiencies. Low-income seniors are at particular risk: about 30% of older adults with lower incomes have lost all their teeth, compared to roughly 12% in wealthier groups.
- Intergenerational Effects: Children with significant tooth decay may struggle in school due to pain or absences, and the cycle can continue if families lack the resources or knowledge to prioritize prevention.
In short, poor oral health exacerbates existing inequities, often compounding chronic diseases, reducing quality of life, and perpetuating disadvantage across generations.
Effects on Families
Disparities in oral health affect entire households, not just individuals.
- Missed School and Work: Dental issues lead to an estimated 320 million hours of lost school and work each year. Low-income parents often lack paid time off, intensifying the economic impact if a child needs urgent dental care.
- Financial Strain: Unexpected dental bills can push already tight budgets into crisis. Some families go into debt or forego other essentials to cover emergencies, orthodontics, or dentures.
- Social and Emotional Impacts: Poor oral health can hinder job prospects, cause embarrassment, and foster social isolation. About 30% of low-income adults feel their dental condition affects their ability to interview confidently for work.
Children in these households may also inherit similar oral health challenges if preventive habits and resources remain limited.
Effectiveness of Public Programs
Government-funded programs and policies have had measurable success, especially for children, though adult coverage remains inconsistent.
- Medicaid/CHIP (Children): Mandatory dental benefits have lowered rates of untreated decay among low-income minors. Half of the children enrolled in Medicaid/CHIP now receive at least one dental service each year, reflecting progress in pediatric outreach.
- Optional Adult Benefits: Where states choose to offer comprehensive adult dental benefits, Medicaid recipients show higher utilization of preventive and restorative care, along with fewer ER visits. However, many states still restrict coverage to emergency extractions, limiting long-term positive impact.
- Community Health Centers: Federally Qualified Health Centers (FQHCs) have expanded dental capacity, improving access in underserved regions. Yet demand often outstrips supply, creating waiting lists and service gaps.
- Preventive Initiatives: Programs like school-based sealants, community water fluoridation, and targeted outreach in WIC or Head Start settings have collectively prevented large numbers of cavities in children and saved millions in future treatment costs.
Despite notable gains, particularly for kids, large gaps remain for low-income adults due to variable policy approaches and funding constraints.
Success Rates of Interventions
Numerous interventions have emerged over the last decade to address socioeconomic disparities, often with promising outcomes.
- School-Based Sealant Programs: These have prevented an estimated hundreds of thousands to a million cavities among low-income children. The protective effect on back teeth can reduce cavities by up to 80% in treated molars.
- Community Water Fluoridation: Reduces tooth decay by approximately 25% for people of all ages while offering a clear economic return (around $20 saved in dental treatments for every $1 invested).
- Medicaid Expansion and Adult Benefits: States that include dental benefits for adults report a 14% drop in emergency dental visits, indicating expanded coverage directs patients toward appropriate, less costly treatment settings.
- Mobile Clinics and Tele-dentistry: Bringing care directly into underserved neighborhoods has improved preventive service uptake. Pilot programs note reductions in untreated decay when clinicians address problems on-site and follow up digitally.
To further reduce the oral health gap, experts emphasize ongoing investment in proven, community-focused strategies that blend coverage, prevention, and education.
Final Summary
The statistics reviewed here underscore how socioeconomic status remains a central determinant of oral health in the United States. Low-income families and those with limited education face higher rates of cavities and tooth loss, fewer preventive visits, and more frequent reliance on emergency departments for pain relief.
Notably, public programs like Medicaid, CHIP, community sealant initiatives, and water fluoridation have driven improvements, especially among children in low-income areas. However, adult coverage remains fragmented, and many individuals still cannot afford or access needed dental care.
These data show that comprehensive, sustained efforts are essential as policymakers and health organizations seek to broaden oral health equity. Addressing cost barriers, expanding provider availability in underserved areas, and prioritizing preventive strategies can help bridge the persistent gap in oral health outcomes between low-SES groups and more affluent populations.
By building on the success of targeted interventions and continuing to fund effective programs, the nation can move closer to ensuring that everyone, regardless of income or education, enjoys a healthier smile and improved overall well-being.
Sources
- CareQuest Institute for Oral Health – https://www.carequest.org/about/press-release/new-report-685-million-adults-us-dont-have-dental-insurance-may-rise-914
- Centers for Disease Control and Prevention (CDC) – Health Disparities in Oral Health – https://www.cdc.gov/oral-health/health-equity/index.html
- Centers for Disease Control and Prevention (CDC) – Health and Economic Benefits of Oral Disease Interventions – https://www.cdc.gov/nccdphp/priorities/oral-disease.html
- Centers for Disease Control and Prevention (CDC) – Unmet Need for Health Care – https://www.cdc.gov/nchs/hus/topics/unmet-need.htm
- Healthcare Cost and Utilization Project (HCUP) – Dental-Related ED Visits – https://hcup-us.ahrq.gov/reports/statbriefs/sb280-Dental-ED-Visits-2018.pdf
- Kaiser Family Foundation (KFF) – Variation in Use of Dental Services by Children and Adults Enrolled in Medicaid or CHIP – https://www.kff.org/medicaid/issue-brief/variation-in-use-of-dental-services-by-children-and-adults-enrolled-in-medicaid-or-chip/
- National Library of Medicine (NIH/PMC) – Disparities in Access to Oral Health Care – https://www.ncbi.nlm.nih.gov/pmc/articles/PMC7125002/
- National Library of Medicine (NIH/PMC) – Orthodontic Treatment Completion and Discontinuation in a Rural Sample – https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5524769/
- The Pew Charitable Trusts – Oral Health Status Has Improved for Children – https://www.pewtrusts.org/en/research-and-analysis/articles/2020/02/24/oral-health-status-has-improved-for-children-but-some-gaps-in-treatment-access-persist

Web content writer specializing in making dental research accessible to diverse audiences.
Related Articles

Best Foods for Healthy Teeth and Gums
What you eat plays a crucial role in maintaining a healthy mouth, and below we cover the best foods to incorporate into...

Best Natural Remedies for Treating Gum Disease
Having a good oral care routine is a great way to prevent gum disease and build the foundation for healthy gums. But the...
How Does Dental Anxiety Affect Your Oral Health?
Dental anxiety (everything from mild nervousness to severe dental phobia) affects a significant portion of the populatio...

What Causes Edentulism?
Edentulism (tooth loss) is a condition that can affect your overall health and quality of life. There are various causes...