Current Orthodontic Treatment Trends & Statistics
Reader-supported. We may earn a commission from links on this page. Advertising disclosure.
In this article
Orthodontic treatment in the United States has changed significantly over the past decade, driven by new technologies and shifting patient demographics.
From discreet treatment options to a growing number of adult patients, orthodontic care continues to evolve in ways that broaden accessibility and improve outcomes.
Orthodontics has long been associated with adolescents wearing traditional metal braces, but it now covers a wide spectrum of ages, socioeconomic backgrounds, and technological approaches.
Below, we cover recent trends and statistics related to orthodontic treatment in the United States, including data on who seeks care, preferred treatment types, average costs, coverage patterns, and completion rates.
Key Statistics to Note
- Roughly one-third of orthodontic patients today are adults, up from about 20% in the early 2000s.
- Clear aligners account for about 30% of new orthodontic case starts, a share that has risen notably over the last 10 years.
- Typical treatment costs hover around $5,000 to $6,000 for both traditional braces and clear aligners, though costs vary by region.
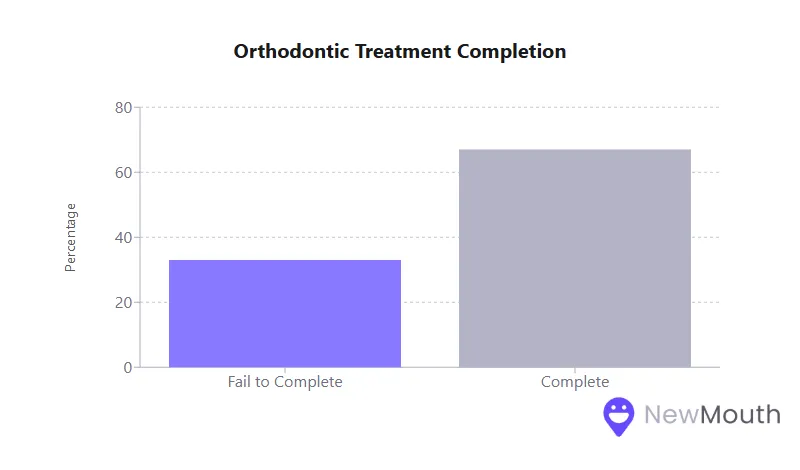
- Completion rates can be as low as 50% in certain clinical settings, with non-completion often tied to financial issues, poor oral hygiene, or lack of patient motivation.
Prevalence of Orthodontic Care
Understanding how common orthodontic treatment is and who receives it provides essential context for broader health and social implications.
- In the United States, millions of children and teens undergo orthodontic care each year, reflecting a longstanding cultural norm of addressing misalignments in adolescence.
- Recent surveys show that about 7 to 8% of children ages 8 to 17 are in active treatment at any given time.
- A significant shift toward adult treatment has emerged over the past decade, indicating that orthodontic care is no longer seen as strictly for children and teenagers.
While many younger patients still initiate orthodontics in early adolescence (around 11 to 14), more adults now recognize the functional, health, and aesthetic benefits of a well-aligned smile. This has shaped provider practices to better accommodate a diverse patient population, from second-graders to retirees.
Age Group Distribution and the Rise of Adult Treatment
Age distribution highlights where the greatest expansion and changes are happening, particularly with adults who are increasingly willing to straighten their teeth later in life.
- Children and Teens
- They continue to make up the largest share of orthodontic patients overall.
- Many start treatment between ages 11 and 15, though early interventions can begin as young as 7 for specific needs (cross bites, severe crowding, or jaw discrepancies).
- Adults
- About one in three current orthodontic patients is over 18, the highest proportion on record.
- Aesthetic appliance options (e.g., clear aligners, ceramic brackets) significantly encourage adult participation, as these are more discreet than traditional metal braces.
- Adults cite reasons beyond cosmetics, including better oral health, easier teeth cleaning, and prevention of future dental complications.
For many adults, modern aligners and ceramic braces have dissolved the old stigma of “metal mouth,” allowing treatment without drawing unwanted attention. This demographic transformation has influenced orthodontic practices to offer expanded office hours, flexible financing, and digital treatment tools that fit busy adult lifestyles.
Clear Aligners vs. Traditional Braces
A major trend in the last 5 to 10 years has been the growing popularity of removable, nearly invisible aligners alongside the longstanding use of bracket-and-wire systems.
- Clear Aligners
- Once considered a specialty option, aligners now comprise about 30% of new case starts in many practices.
- They often reduce overall treatment time by a few months compared to braces, especially in mild to moderate cases.
- Patients report high satisfaction due to removable trays (easier oral hygiene, unrestricted diet) and discreet appearance.
- Traditional Braces
- Still represent the majority of new starts (about 70% in recent surveys), especially for complex cases or younger teenagers.
- Offer predictable, full-range tooth movement for severe issues.
- Come in multiple variants: metal brackets (most common), ceramic (clear) brackets, and lingual braces (on the back of the teeth).
Although aligners are closing the gap, traditional braces remain indispensable for comprehensive corrections. Many orthodontists combine approaches. Some patients start with braces to address complex movements and then switch to aligners for the finishing phase.
Comparing Treatment Costs Across the USA
Costs are a crucial factor for many families and adults, influencing choices about whether, when, and how to pursue treatment. Though fees vary by region and complexity, national averages have converged between aligners and traditional braces.
| Treatment Type | Average Total Cost | Typical Range |
|---|---|---|
| Metal Braces | $5,000 to $6,000 | $3,000 to $7,000 |
| Ceramic Braces | $5,000 to $6,500 | $4,000 to $8,000 |
| Lingual Braces | $6,000 to $8,000 | $5,000 to $13,000 |
| Clear Aligners | $5,000 to $6,000 | $1,500 to $10,000 |
- Regional Variations
- Major urban and coastal areas (e.g., New York, California) can see aligner fees as high as $6,000 to $7,000 or more.
- Some Midwestern or Southern states offer lower fees, occasionally under $4,000 for moderate aligner cases.
- Similar Averages
- Recent nationwide data show the average comprehensive braces treatment fee is around $6,000, with clear aligners close behind at about $5,900 to $6,000.
With both modalities converging on similar price points, many patients now choose based on comfort, aesthetics, and lifestyle preferences rather than cost alone.
Insurance Coverage and Affordability
Dental insurance plays a major role in expanding or limiting access to orthodontic care. Many private plans offer partial coverage, but the specifics vary widely.
- Typical Coverage Structure
- Often covers 50% of treatment up to a lifetime maximum, frequently in the range of $1,500 to $3,000.
- Higher-end or “upgrade” appliance fees (like lingual braces) might fall outside standard coverage in some plans.
- Children vs. Adults
- Many employer-sponsored dental plans restrict orthodontic benefits to minors under age 19.
- Adult ortho coverage exists but is less common, leaving many adults to pay out-of-pocket or rely on flexible spending accounts.
- Medicaid/Public Insurance
- Coverage is available for children when deemed medically necessary (e.g., severe malocclusion).
- Rarely covers adult orthodontics unless there is a surgical or critical health need.
- Disparities persist; children covered by Medicaid often face reduced provider availability, and their completion rates can be lower due to socioeconomic challenges.
Overall, out-of-pocket expenses remain significant for a large segment of the population, illustrating why socioeconomic factors heavily influence who can afford orthodontics.
Typical Treatment Duration
While orthodontic treatment still takes 18 to 24 months for comprehensive correction, technological and planning advances have helped reduce the time for certain cases.
- Braces
- Standard comprehensive care: ~2 years (sometimes up to 30 months).
- Complex corrections (severe crowding, jaw misalignment) can take longer, though improved bracket designs and wires may speed some aspects.
- Clear Aligners
- Typical completion in 12 to 18 months for mild to moderate issues, though this can extend if refinements are needed.
- Studies comparing braces and aligners show aligners can be up to ~6 months faster in cases of similar complexity.
Despite these averages, biology is still a limiting factor: teeth move at a certain pace, and attempts to drastically accelerate tooth movement risk complications. For many patients, consistent wear of appliances and diligent oral care remain the biggest influences on final treatment length.
Effectiveness and Success Rates
Orthodontic treatments generally enjoy high success rates in achieving straighter teeth and more functional bites, provided patients comply with instructions and complete the process.
- Traditional Braces
- Considered the gold standard for all severities of misalignment.
- Success rates can exceed 90% when patients attend appointments and follow instructions (e.g., wearing elastics).
- Clear Aligners
- Extremely effective (80 to 90% success) for mild to moderate cases.
- Comparable end results to braces in terms of alignment and bite quality, though braces may be more precise for very complex movements.
- Heavily reliant on patient adherence; aligners must be worn ~22 hours per day.
To maintain these results, consistent retainer wear after treatment is essential. Even high-quality orthodontic work can relapse if patients abandon their retainers.
Patient Satisfaction Measures
Patient satisfaction goes beyond the final smile. It encompasses comfort, aesthetic concerns, convenience, and the overall experience during treatment.
- High Satisfaction with Clear Aligners
- Studies show 85% or more of aligner patients report positive experiences.
- Trays are nearly invisible, and patients can remove them to eat or brush, boosting comfort and confidence.
- Experience with Braces
- Though effective, braces can irritate the inside of the mouth, limit food choices, and require careful hygiene to prevent plaque buildup.
- Still, many braces patients are ultimately highly satisfied, especially once they see the end results.
Improvements to braces technology, including ceramic brackets or smaller metal brackets, have partially narrowed the comfort and aesthetic gap. In either scenario, patient perception of the appliance often improves over time as they adapt and observe teeth gradually moving into alignment.
The Technological Transformation in Orthodontics
Digital technology has reshaped the orthodontic workflow from initial diagnosis to final retainer checks.
- Intraoral Scanners
- Replacing messy physical impressions, digital scans capture exact tooth positions in minutes.
- Models can be exported instantly for aligner fabrication or 3D-printed appliances.
- AI-Driven Treatment Planning
- Sophisticated software simulates tooth movement in steps, helping orthodontists design precise bracket placements or aligner sequences.
- Artificial intelligence refines force distributions and staging to optimize efficiency.
- Remote Monitoring
- Patients can upload progress photos or scans, letting providers track tooth movement without frequent office visits.
- This has reduced in-person appointments from every 6 weeks to every 10 or 12 weeks for many aligner patients, saving time and resources.
Such innovations have boosted convenience and accuracy, allowing orthodontists to deliver personalized care that can be digitally assessed and adjusted in real time.
Socioeconomic Disparities in Orthodontics
Despite technological advances, access remains uneven. Orthodontic care strongly correlates with household income and insurance status.
- Higher-Income Households
- Far more likely to utilize orthodontic services, often with private insurance coverage.
- Have higher completion rates, as financial difficulties rarely interrupt treatment.
- Low-Income and Minority Populations
- Face challenges such as reduced insurance coverage, fewer orthodontists accepting Medicaid, and logistical hurdles (transportation, missed work).
- Show lower uptake of orthodontic treatment and higher dropout rates when treatment is initiated.
Professional associations are attempting to expand coverage for underserved groups. They argue that misaligned teeth can negatively impact oral health, social confidence, and long-term quality of life.
Early Intervention (Phase I) Treatment
Early or interceptive orthodontic treatment (often around ages 7 to 10) aims to address jaw growth issues or severe crowding before all permanent teeth erupt.
- Objectives
- Correct crossbites or significant skeletal discrepancies.
- Reduce the need for extractions or jaw surgery later.
- Potentially shorten the second treatment phase during the early teen years.
- Utilization
- An estimated 10 to 15% of children get some form of Phase I care, often involving a palatal expander, partial braces, or habit appliances.
- Overly broad use of two-phase treatment has declined compared to the 1990s, as research suggests comprehensive adolescent treatment alone can suffice for many cases.
When indicated, early intervention can produce measurable long-term benefits. However, orthodontists today often take a conservative approach, reserving Phase I for clear, specific needs rather than a universal two-phase plan.
Completion Rates and Patient Adherence
An under-discussed issue in orthodontics is that not all patients who start treatment finish it as prescribed.
- Discontinuation Rates
- Research indicates one-third or more of patients in some settings fail to complete treatment.
- Common reasons: financial strain, relocation, poor oral hygiene, or patient frustration with the process.
- Adherence Factors
- For aligners, compliance means wearing trays ~22 hours per day. Skimping on wear time prolongs treatment or derails progress.
- For braces, patients must maintain strict oral hygiene and follow elastics/headgear protocols.
- Missed appointments and unwillingness to follow instructions can lead providers to end treatment prematurely.
Orthodontic offices increasingly use motivational approaches, like apps, text reminders, or reward systems, to improve follow-through, reinforcing that success hinges on patient engagement as much as professional skill.
Final Summary
Orthodontic treatment in the United States is thriving, with growing numbers of children, teens, and adults embracing it. Technological advances have attracted new demographics, including image-conscious adults who once hesitated to get braces.
Despite these positive developments, cost barriers, insurance limitations, and socioeconomic inequities remain significant obstacles. Additionally, some patients discontinue treatment before achieving their goals, illustrating the importance of consistent follow-up and adherence.
Looking ahead, the orthodontic field is poised for further evolution. As digital tools refine treatment planning and remote monitoring becomes more sophisticated, patients can expect greater convenience, and providers can deliver even more personalized care.
Nonetheless, expanding insurance coverage, addressing disparities, and sustaining patient motivation will remain integral to ensuring that orthodontics benefits all who need it. In the end, orthodontic care has proven capable of transforming not just smiles but self-confidence and overall oral health.
Sources
- American Association of Orthodontists (AAO) – https://aaoinfo.org/blog/number-of-adults-seeing-an-orthodontist-is-at-an-all-time-high
- Frontiers – Orthodontic Treatment Completion and Discontinuation in a Rural Sample from North Central Appalachia in the USA – https://www.frontiersin.org/journals/public-health/articles/10.3389/fpubh.2017.00171/full
- Orthodontic Practice Performance Survey (2022) – https://orthodonticproductsonline.com/practice-management/business-development/2022-orthodontic-practice-performance-survey
- Spirit Dental – Costs for Common Dental Procedures – https://spiritdental.com/blog/categories/procedures/costs-for-common-dental-procedures

Web content writer specializing in making dental research accessible to diverse audiences.
Related Articles

Best Foods for Healthy Teeth and Gums
What you eat plays a crucial role in maintaining a healthy mouth, and below we cover the best foods to incorporate into...

Best Natural Remedies for Treating Gum Disease
Having a good oral care routine is a great way to prevent gum disease and build the foundation for healthy gums. But the...
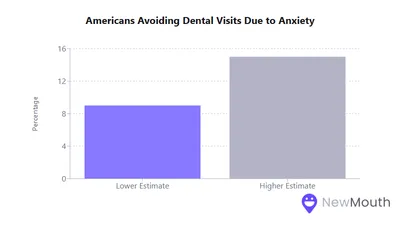
How Does Dental Anxiety Affect Your Oral Health?
Dental anxiety (everything from mild nervousness to severe dental phobia) affects a significant portion of the populatio...
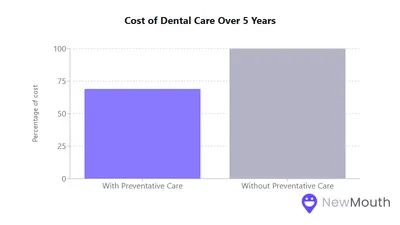
Dental Care Spending: Statistics and Trends
Dental expenditures in the United States have steadily risen over the past decade, reflecting shifts in procedure costs,...