Mandible Bone (Lower Jaw): Anatomy, Function, and Common Problems
Reader-supported. We may earn a commission from links on this page. Advertising disclosure.
In this article
Mandible Bone (Lower Jaw): Anatomy and Function
The mandible is the lower jawbone. It holds your bottom teeth, gives shape to the lower face, and moves at the TMJ so you can chew, speak, and yawn.1 Problems affecting the mandible include fractures, TMJ disorders, dislocation, and jaw misalignment.
Mandible Bone Quick Facts
- What is the mandible bone? The lower jawbone — the largest and strongest bone of the face, and the only movable skull bone besides the tiny middle-ear bones.2
- What problems affect the mandible? Fractures, TMJ disorders, dislocation, jaw misalignment, and (rarely) osteomyelitis.
- What’s the difference between the jaw and the mandible? “Jaw” refers to both upper and lower; the mandible is only the lower portion. The maxilla forms the upper jaw and stays fixed to the skull.
- What’s another name for the mandible? Lower jaw, lower jawbone, or mandibular bone.
What Are the Primary Functions of the Mandible?
The mandible’s main job is to move the jaw for chewing (mastication) and speaking. It houses the lower set of teeth and provides passage and attachment for nerves, blood vessels, and muscles that travel through, into, and out of the bone.1
What Problems Can Affect the Lower Jaw?
The lower jaw is prone to a small set of disorders that affect how it moves, fits, and feels. These include:
Jaw Fractures
A broken mandible usually shows up as pain that worsens when you chew or speak, a bite that suddenly feels off, and sometimes a visible shift in the jawline. Most mandibular fractures happen during car crashes, falls, sports collisions, and assaults.3
Treatment depends on where the break is and how the pieces sit. Some fractures heal with manual repositioning and a short period of restricted jaw movement. Others need jaw surgery with plates and screws to hold the bone in place.3
Jaw Misalignment
A misaligned jaw makes your upper and lower teeth meet wrong, and over time that mismatch causes uneven tooth wear, jaw pain, and trouble chewing or speaking.4 Some people are born with jaw misalignment; others develop it from facial trauma or long-term habits like prolonged thumb sucking.
Treatment options include:
- Orthodontic treatment (braces or clear aligners) for milder cases
- Orthognathic surgery for severe skeletal mismatch, usually combined with braces5
- Physical therapy to address jaw muscle pain that accompanies the bite issue
Dislocations
A dislocated jaw usually locks your mouth open — you cannot close it on your own. If only one side is dislocated, the jaw tends to shift toward one side; if both sides are dislocated, it stays open and roughly centered. The lower jaw typically slips forward out of the temporomandibular joint, sometimes after a wide yawn, a dental procedure, or facial trauma.6
A dislocated jaw usually needs prompt reduction by a clinician, who manually guides the joint back into place. Traumatic, fracture-associated, chronic, or nonreducible dislocations may need oral-maxillofacial or emergency care.6
Temporomandibular Joint Disorders (TMD)
TMD is a common jaw disorder that affects the temporomandibular joint and the muscles around it.7 Symptoms include:
- Jaw pain and stiffness
- Difficulty chewing
- Headaches and earaches
- Lockjaw
- Jaw popping or clicking
Painless clicking on its own is common and usually does not need treatment. When pain or limited motion is present, conservative care comes first — jaw rest, soft foods, heat, gentle stretching, and sometimes a custom night guard. Experts strongly recommend trying these before any permanent bite changes or surgery.7
Sleep Apnea
Sleep apnea is a sleep disorder in which breathing repeatedly stops or shrinks during sleep. Common signs include loud snoring, gasping for air at night, and daytime sleepiness.8 Sleep apnea and TMD can overlap, but researchers have not established a simple one-way cause-and-effect relationship between them.9
If you have TMD symptoms along with loud snoring, witnessed breathing pauses, or daytime sleepiness, ask your dentist or doctor for a sleep evaluation referral. Because the link between TMD and sleep apnea is still being studied, each condition is best evaluated and treated on its own.
Osteomyelitis and Bone Disintegration
Osteomyelitis is a bone infection that reaches the mandible through a dental abscess, an invasive oral procedure, or a jaw fracture that breaks the skin. Common warning signs include persistent or worsening jaw pain, facial swelling or tenderness, fever, drainage or pus, jaw stiffness, and trouble eating or speaking.10
Untreated osteomyelitis damages jawbone tissue and, in some cases, leads to tooth loss or drainage from the infected area. Treatment usually includes a long course of antibiotics, and severe or unresponsive cases also need drainage or surgery to remove dead bone.10
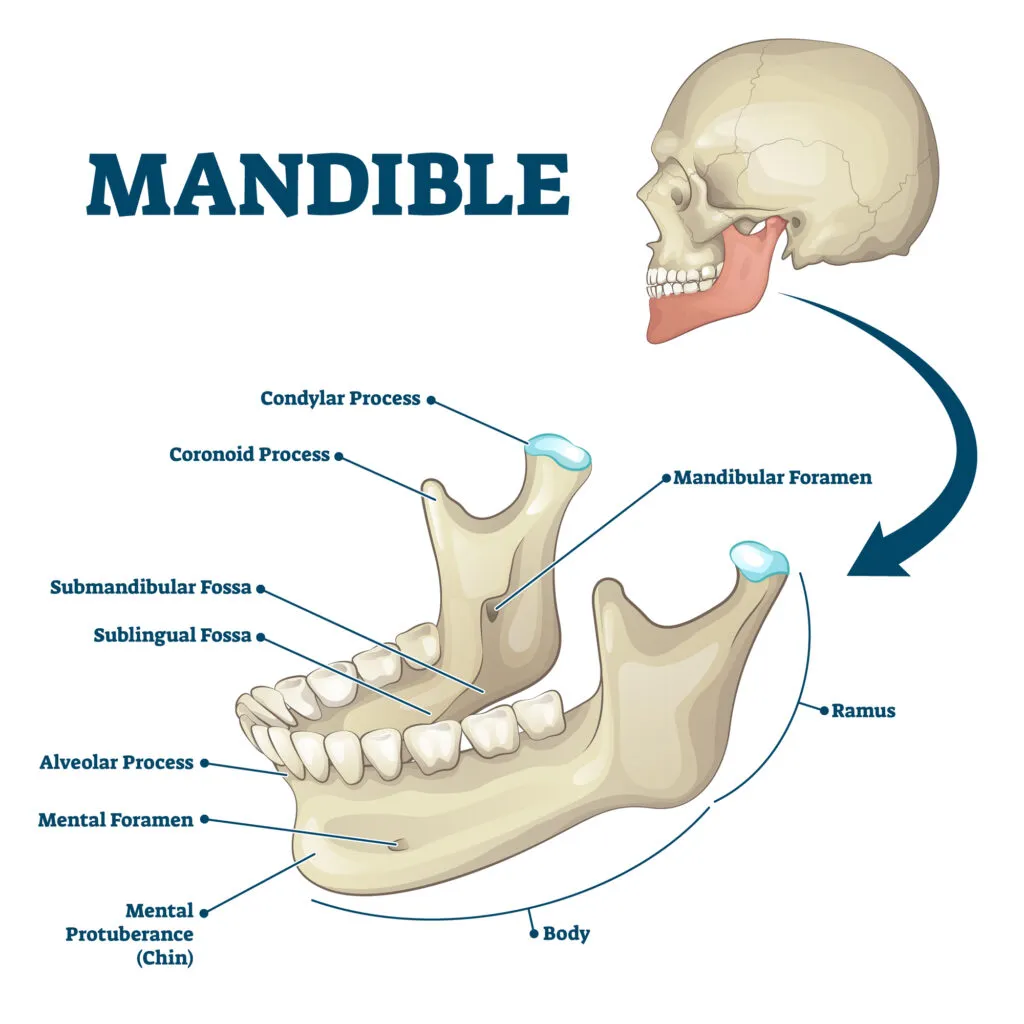
Mandible Anatomy and Structure
The mandible sits directly below the upper jaw and consists of a horseshoe-shaped body with two vertical extensions called rami. The body forms the lower jawline, and a ramus rises from each end of the body to meet the skull at the TMJ.1
Male mandibles are generally larger than female mandibles, with more pronounced muscle attachment points.11
Below are the parts that make up the mandible:
Body
The body of the mandible forms your chin and jawline. It is a curved, roughly rectangular bone that lies horizontally across the lower face, with a subtle midline ridge called the mandibular symphysis on its external surface.1
The body’s alveolar border — the upper surface — is where the 14 to 16 lower teeth attach, depending on third-molar status.1
Ramus
The ramus is the vertical part of the jaw that rises from each end of the body. It is the second-largest part of the mandible and meets the body at the gonial angle.1
The gonial angle varies with age and sex.11
Each ramus consists of the following parts:
- Head — Connects with the temporal bone to form the TMJ.
- Neck — Supports the head and serves as the attachment point for the lateral pterygoid muscle at the pterygoid fovea.
- Coronoid process — The attachment site for the temporalis muscle, which generates jaw movement at the TMJ.
Alveolar Process
The alveolar process is the part of the mandible that holds your teeth in place via a joint called a gomphosis.12 It extends upward from the mandibular body and is made of two bony plates that form the tooth sockets.
Each side of the mandible holds five primary teeth during childhood and seven to eight permanent teeth in adults, depending on whether wisdom teeth are present.12
Mandibular Foramen and Mental Foramen
The mandibular foramen is an opening on the inner surface of the ramus that leads into the mandibular canal. The inferior alveolar nerve, artery, and vein enter there and travel forward through the canal toward the mental foramen.1
The mental foramen sits on the outer surface of the mandibular body between the first and second premolar. The mental nerve emerges here with its accompanying blood vessels and supplies sensation to the lower lip and chin.1
Other Jaw Structures
The mandible is the skeletal frame of the lower jaw. The soft-tissue structures that work alongside it include:
Blood and Lymph Vessels
The mandible receives blood from small periosteal and endosteal vessels that branch off surrounding arteries. The lower teeth get their blood supply from dental branches of the inferior alveolar artery.1
Lymphatic fluid from the mandible and lower teeth drains primarily through the submandibular lymph nodes.1
Nerves
The main nerve that supplies the mandible is the inferior alveolar nerve, a branch of the mandibular division of the trigeminal nerve.1
The inferior alveolar nerve enters through the mandibular foramen and runs forward through the mandibular canal, sending branches to the lower teeth as it goes. At the mental foramen, it splits into two terminal branches:
- Mental nerve — Exits through the mental foramen to give sensation to the lower lip and chin.
- Incisive nerve — Continues through the incisive canal to supply the lower central and lateral incisors, canines, and premolars.1
Muscles
Several muscles attach to the mandible to drive chewing, swallowing, and facial expression.13 The primary muscles include:
- Masseter — Inserts into the ramus and is one of the strongest chewing muscles.
- Temporalis — A fan-shaped muscle along the side of the head that helps close the jaw.
- Medial pterygoid — A thick, rectangular muscle that assists chewing and elevates the jaw.
- Lateral pterygoid — Moves the jaw downward and side-to-side.
- Mylohyoid — Forms the floor of the mouth.
- Buccinator — Originates from the alveolar process and assists in chewing by pressing food against the teeth.
- Superior pharyngeal constrictor — Connects to the mylohyoid and helps drive swallowing.
When to See a Dentist or Doctor
Most jaw symptoms do not need emergency care, but a few warning signs warrant same-day attention:
- Inability to close your mouth or visible jaw deformity after trauma. A possible dislocation or fracture needs urgent reduction or repair.3,6
- Persistent or worsening jaw pain with fever, swelling, drainage, or pus. These are warning signs of jaw osteomyelitis or a deep dental infection.10
- Loud snoring with witnessed breathing pauses, gasping, or daytime sleepiness. Ask your doctor or dentist about a sleep evaluation for possible sleep apnea.8
- Ongoing jaw pain, clicking with pain, or limited mouth opening. A dentist familiar with TMD can guide you through conservative care before any permanent bite changes are considered.7
For many TMD symptoms, simple conservative care is the first step, and your general dentist is a reasonable first call. Early evaluation is usually simpler and more effective than waiting for symptoms to worsen.
The Mandible Lower Jaw
NewMouth PodcastSources
- Breeland, Grant, et al. “Anatomy, Head and Neck, Mandible.” StatPearls, 2023.
- “Mandible.” National Cancer Institute Dictionary of Cancer Terms, nd.
- “Facial Injury / Trauma Surgery.” American Association of Oral and Maxillofacial Surgeons, 2021.
- “Overview: Misaligned Teeth and Jaws.” Institute for Quality and Efficiency in Health Care, 2023.
- “Corrective Jaw Surgery.” American Association of Oral and Maxillofacial Surgeons, nd.
- Hillam, Joshua, et al. “Mandible Dislocation.” StatPearls, 2023.
- “TMD (Temporomandibular Disorders).” National Institute of Dental and Craniofacial Research, nd.
- “What Is Sleep Apnea?” National Heart, Lung, and Blood Institute, 2025.
- Rigon, Marcelo, et al. “Relationship Between Temporomandibular and Sleep Disorders in Adults: An Overview of Systematic Reviews.” Sleep Medicine, 2024.
- Furto, Eric S. “Physical Therapy Guide to Osteomyelitis of the Jaw.” ChoosePT, 2023.
- Vinay, G, et al. “Sex Determination of Human Mandible Using Metrical Parameters.” Journal of Clinical & Diagnostic Research, 2013.
- National Library of Medicine. “Alveolar Process.” Medical Subject Headings, D000539.
- Basit, Hajira, et al. “Anatomy, Head and Neck, Mastication Muscles.” StatPearls, 2023.

UCLA-trained dentist practicing in public health. Focuses on whole-body approach to dental care.

Experienced dental health writer dedicated to providing accurate, accessible information.
Related Articles

Black Triangles Between Your Teeth
When you look in the mirror, you may notice small black triangles between your teeth. These are gaps that your gum tissu...

Bleeding Gums: Causes, Remedies & Treatment
Bleeding gums can be a sign of gum disease. They can also be caused by other things like brushing too hard or hormonal c...

Botox For Bruxism
Teeth grinding or bruxism causes pain, discomfort, and even sleep deprivation. Fortunately, there is an effective treatm...

Bruxism (Teeth Grinding)
Clenching or grinding your teeth during sleep is called bruxism. Here's what you need to know, including treatment optio...