What Are Dentistry Challenges in Developing Countries?
Reader-supported. We may earn a commission from links on this page. Advertising disclosure.
In this article
Oral health needs are vast worldwide, yet many regions lack the policies, infrastructure, and resources necessary to ensure quality dental care for all. This gap is especially evident in low- and middle-income nations across Africa, Asia, and Latin America, where economic and geographic constraints often prevent significant segments of the population from ever seeing a dentist.
By exploring the complex challenges facing dental healthcare in developing countries and notable areas of progress, we gain insight into how targeted investments and strategic reforms can gradually close the gaps in oral health equity.
The following sections review key statistics and trends shaping the dental landscape in these regions, including critical data on workforce, costs, prevention, government programs, and inequalities that persist despite ongoing efforts.
Noteworthy Statistics
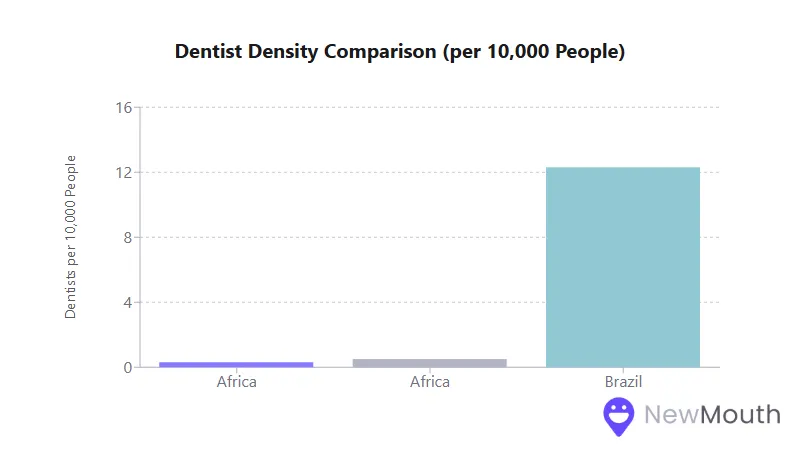
- The average in many parts of Africa is 0.3 to 0.5 dentists per 10,000 people, the lowest regional density in the world.
- In India, the supply of dentists nearly doubled between 2012 and 2019, yet 85% of them practice in urban areas where only about 30% of the population resides.
- In Latin America, Brazil has 12.3 dentists per 10,000 people (one of the highest ratios globally), but large rural or low-income populations still have limited access to care.
- Out-of-pocket payments for dental services exceed 70% of total dental spending in numerous developing countries, making routine treatments financially unattainable for millions.
The Importance of Understanding Global Dental Challenges
A clear picture of the dental workforce, care availability, and infrastructure in developing regions is essential for guiding policy decisions and health interventions. Many of the same factors, such as health financing, preventive coverage, and training capacity, determine whether communities can access basic oral healthcare or must seek unqualified alternatives.
By examining these factors in detail, stakeholders can better address the root causes of poor dental outcomes and allocate resources where they are needed most.
Below, we examine how workforce shortages, cost barriers, and weak national programs collectively restrict the reach of modern dentistry across various developing contexts. These sections also explore how certain countries’ reforms and preventive strategies are making strides in reducing dental disease, particularly among children and other vulnerable groups.
Workforce Challenges
In many developing regions, the sheer shortage of dental professionals remains a fundamental barrier to improving oral health. This deficit is most pronounced in sub-Saharan Africa, where average dentist density can hover around 0.3 to 0.5 dentists per 10,000 people, far below the minimum thresholds recommended by global health agencies.
Even countries with stronger training pipelines often battle “brain drain,” as new graduates migrate to wealthier nations or cluster in major cities.
- In parts of Africa, some nations have 1 dentist per 1 million people, effectively none in practical terms.
- South Asian countries like Pakistan and Bangladesh report fewer than 0.6 dentists per 10,000, leaving rural districts with little or no coverage.
- Even when the raw number of dentists improves, such as in India, which now graduates tens of thousands of dentists annually, 85% or more of these providers remain in urban regions.
- Latin America, by contrast, can produce relatively high densities in large cities (e.g., Argentina, Mexico), yet isolated provinces and indigenous communities remain chronically underserved.
This maldistribution, whether caused by economic incentives, lack of infrastructure, or underinvestment in rural clinics, translates into limited primary dental care for huge swaths of the population.
Without policies or financial incentives encouraging rural or community service, newly trained dentists typically concentrate where facilities, equipment, and paying patients are most plentiful. The end result is urban clusters of private clinics and persistent neglect of remote or low-income areas.
Access and Financial Barriers
Out-of-Pocket Costs
Across Africa, Asia, and Latin America, out-of-pocket payments for dental treatments can exceed 70% of total dental spending, making even routine procedures like fillings, cleanings, or tooth extractions prohibitively expensive.
In many low-income settings, per capita government spending on oral health stands at less than US $1 per year, insufficient to staff or equip public dental clinics. As a consequence:
- Poor and rural households often delay or forego dental care, waiting until pain becomes severe.
- In Africa, where national insurance rarely covers oral health, catastrophic expenses are a real risk if more complex treatment is needed.
- In South Asia, large informal labor sectors leave many outside formal insurance schemes, so most pay for dental services entirely out of pocket.
- While Latin America has more public dental programs in certain countries, significant segments of the population in countries like Mexico or Peru still struggle to afford private visits.
Because simple dental issues become emergencies without early intervention, low-income groups are disproportionately affected by complications like advanced decay or infections. This drives up overall healthcare costs and leads to tooth extractions rather than affordable conservative care.
Countries that have integrated basic dental treatments into national health programs, like Thailand or parts of Brazil, illustrate how coverage can boost utilization and reduce financial strain.
Infrastructure Gaps
Even where services are nominally available, many government-run clinics in remote areas lack consistent electricity or modern equipment like X-ray units, sterilizers, or high-speed dental drills.
Maintaining donated machines is also a challenge; if they break, replacement parts or trained technicians may be scarce. The net effect is that clinics can perform only basic procedures (often extractions) without the capacity for root canals, restorative treatments, or more advanced care.
Meanwhile, urban private practices in middle-income countries may feature the latest technology, from digital imaging to dental implants. This dichotomy heightens equity concerns: one segment of society enjoys world-class dentistry while the poor contend with limited or no care.
Closing this equipment gap will require strategic public-private partnerships, better supply chains, and a focus on ensuring continuous maintenance and training.
Community Prevention
Effective prevention programs are the hallmark of any successful oral health system, yet in many low-resource settings, these remain underdeveloped. A lack of awareness, insufficient budgets, and limited political commitment hinder large-scale interventions that could curb rising dental disease.
- Water or Salt Fluoridation: In parts of Latin America, extensive salt fluoridation campaigns have led to significant drops in childhood cavities. Similarly, some Southeast Asian countries (e.g., Thailand) maintain regional water fluoridation or have considered fluoridated salt. Many African and South Asian nations have yet to implement these proven preventive strategies broadly.
- School-Based Programs: Thailand has pioneered supervised toothbrushing in schools, while Brazil and Chile have integrated fluoride mouth rinses and regular screenings for students. Such initiatives remain partial or pilot-only in much of Africa and South Asia.
- Behavior Change Education: Simple messages around twice-daily brushing, dietary sugar reduction, and early check-ups can dramatically lower the burden of decay. However, resource constraints limit mass awareness efforts and hamper the distribution of affordable fluoride toothpaste in some regions.
Where these preventive measures are adopted on a large scale, children show markedly lower rates of dental caries. Without them, communities often rely on emergency-driven care. Strengthening prevention could, therefore, ease the workload on overstretched dental services while also helping families avoid the costs and pain of advanced disease.
Progress in National Programs
Some developing countries have made important strides by incorporating oral health into broader universal coverage:
- Brazil’s National Policy (“Brasil Sorridente”) has systematically expanded public dental clinics and created specialized centers, offering free preventive and curative services through the national health system.
- Thailand includes dental benefits within its Universal Coverage Scheme, resulting in higher rates of routine dental visits and school-based prevention.
- Sri Lanka deploys school dental therapists and ensures pregnant women receive basic periodontal checks, a model that shows reduced tooth decay among children and better awareness among mothers.
Meanwhile, certain Latin American nations like Chile and Costa Rica leverage guaranteed dental benefits for youth or older adults, ensuring these vulnerable groups can access essential treatments.
Even in Africa, where oral health budgets are minuscule, some countries (e.g., Rwanda, Kenya) are drafting policies to better integrate dentistry into primary healthcare, though actual implementation remains a challenge.
Programs that emphasize prevention, community outreach, and financial protection demonstrate measurable reductions in untreated decay and tooth loss. The lesson is clear: when governments allocate dedicated funding to dental services, disparities shrink and population outcomes improve.
However, in many low- and middle-income nations, oral health still competes with other pressing priorities (e.g., maternal health, infectious diseases), limiting its slice of the public health budget.
Persistent Inequalities
Despite progress in certain areas, deeply ingrained inequalities continue to define dental health in developing regions. Rural communities, low-income groups, and indigenous populations regularly have:
- Higher rates of untreated decay, gum disease, and edentulism (tooth loss).
- Fewer opportunities for preventive care or early intervention.
- A heavier financial burden when they do seek care, as private options are their main recourse.
In sub-Saharan Africa, the most affluent individuals might travel abroad or to major urban centers for dental procedures, while the average rural resident endures pain or relies on traditional healers.
Similarly, in South Asia, slum dwellers near big cities often cannot afford the private clinics that line more affluent neighborhoods. Latin America’s indigenous populations in mountainous or jungle regions also see far less coverage from national dental programs, despite overall dentist surpluses in some countries.
Gender and cultural factors may amplify these disparities. In certain societies, women may postpone their own oral healthcare, prioritizing limited household funds for other needs. Distrust of medical institutions or strong reliance on folk remedies can further widen the gap between formal and informal treatment options, especially in remote areas.
The Path Forward
Strengthening Prevention and Primary Care
Expanding coverage of population-level fluoridation, school-based screenings, and hygiene education programs can significantly reduce new caries, especially among children.
Ensuring that primary health centers have at least minimal dental capabilities (trained staff, basic materials) could redirect routine cases from overcrowded hospitals and empower earlier interventions. This approach demands political will to allocate steady resources rather than short-term pilot grants.
Improving Workforce Distribution
Encouraging or mandating rural service for newly graduated dentists, backed by adequate pay, housing, or loan forgiveness, has shown results in countries like Thailand, Sri Lanka, and parts of Latin America.
Parallel efforts to train mid-level providers (dental therapists, hygienists) can free dentists to handle more complex work. Offering continuing education and career pathways in underserved regions also improves retention.
Ensuring Financial Protection
Dental services must be integrated into universal health packages where feasible. Countries that have made at least basic or emergency dental care free at the point of use report increased access and reduced catastrophic spending.
Even partial coverage, such as for preventive treatments and simple restorations, creates a powerful incentive for patients to seek care sooner. This is especially relevant in South Asia and Africa, where most people still pay out of pocket in private clinics.
Scaling Up Infrastructure and Technology
Reliable electricity, water supply, and essential dental equipment must be prioritized in public clinics. Beyond big-ticket technology like digital imaging, maintaining autoclaves for sterilization and ensuring steady supplies of anesthetics and filling materials can dramatically improve outcomes.
Partnerships with private companies, NGOs, and international donors could furnish equipment, but local training in equipment maintenance is equally key for long-term sustainability.
Final Summary
In recent years, many developing nations have shown that strategic investments in dental care, especially around prevention, workforce distribution, and financial protection, can yield measurable gains.
From Thailand’s universal coverage model to Brazil’s expanded public clinics, these successes underline the importance of sustained government backing rather than one-off initiatives. Nonetheless, far too many rural and low-income populations still lack adequate dental services, a gap that fuels high rates of untreated decay, painful complications, and avoidable tooth loss.
The good news is that the path to improvement is well established: extend community-based preventive programs, integrate routine dental benefits into broader health systems, and target resources where oral health disparities are most acute.
By consolidating these approaches and building on the encouraging reforms already underway, developing regions can continue to reduce the prevalence of dental disease and ensure that oral healthcare is viewed not as a luxury but as a fundamental element of overall health and well-being.
Sources
- Borgen Project – https://borgenproject.org/oral-health-in-latin-america/#:~:text=3,dominating%20country%20in%20dental%20hygiene
- Frontiers in Oral Health (2025) – Resources for Oral Health in Africa – https://www.frontiersin.org/journals/oral-health/articles/10.3389/froh.2025.1540944/full#:~:text=the%20African%20oral%20health%20workforce
- PAHO/WHO (2023) – Regional Oral Health Report, Americas – https://www.paho.org/en/news/27-10-2023-paho-launches-whopaho-regional-report-state-oral-health#:~:text=Oral%20diseases%27%20prevalence%20in%20the,costs%20for%20individuals%20and%20society
- Times of India (2012) – Dentist Density in India & Neighbors – https://timesofindia.indiatimes.com/india/less-than-one-dentist-for-10000-indians/articleshow/13185257.cms#:~:text=The%20World%20Statistics%202012%2C%20released
- WHO (African Region) – Oral Health Overview – https://www.afro.who.int/health-topics/oral-health#:~:text=Access%20to%20oral%20health%20services

Licensed dental specialist focusing on personalized dental content writing and blogging.

Web content writer specializing in making dental research accessible to diverse audiences.
Related Articles

Best Natural Remedies for Treating Gum Disease
Having a good oral care routine is a great way to prevent gum disease and build the foundation for healthy gums. But the...

Best Dental Loan Options in 2026
Here are some of the best dental loans you can get in 2026: 1. Best Egg Best Egg is an online lending platform that offe...

What is a Dry Socket & What Does it Look Like?
Dry socket can be a painful and uncomfortable dental condition that occurs when a tooth is extracted. This article expla...

Recognizing and Addressing Dental Fistulas
Have you noticed a small bump on your gums that occasionally oozes pus? You might be dealing with a dental fistula. Whil...