Tooth Loss Prevalence Statistics in Seniors: Disparities and Health Impact
Reader-supported. We may earn a commission from links on this page. Advertising disclosure.
In this article
Tooth loss is a crucial oral health concern that disproportionately affects older adults, but it also impacts people across all demographics.
While losing a tooth can seem like a straightforward problem, the data paints a more complex picture: tooth loss influences nutrition, general health, social interactions, and self-esteem.
Over the last 5 to 15 years, researchers have gathered extensive data on tooth loss trends, revealing improvements in some areas and persistent disparities in others.
This article looks at tooth loss prevalence, demographic patterns, treatment options, and long-term outcomes, highlighting both the personal and societal impacts.
Key Statistics at a Glance
- Notable Decline in Complete Tooth Loss: Among U.S. adults aged 65 and over, the prevalence of complete tooth loss dropped from roughly 30% in 2000 to around 13% in more recent years.
- Gender Gap Is Narrowing: In the United States, men and women now have similar rates of complete tooth loss among older adults, although past generations saw higher edentulism in women.
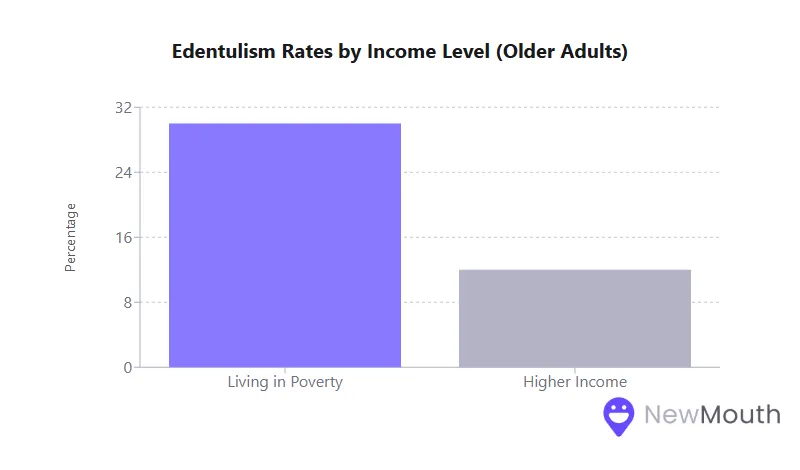
- Socioeconomic Divide: Older adults living in poverty have more than double the rate of edentulism (around 30%) compared to higher-income seniors (around 12%).
- Global Burden: Worldwide, over 350 million people are completely edentulous as of the early 2020s. This figure is projected to exceed 600 million by 2050 due to population aging.
Age-Related Patterns in Tooth Loss
Tooth loss becomes more common with age. The risk of missing multiple teeth rises over time, largely because dental disease adds up over a lifetime.
Examining these statistics clarifies the progress made in preventive dentistry and the ongoing challenges:
- Over the past five decades, complete tooth loss (edentulism) among older Americans (65 to 74) has dropped from around 50% in the 1960s to roughly 13% in the most recent surveys. This improvement reflects broader public health measures, especially water fluoridation and regular dental care, that help people preserve their teeth longer.
- Even so, about 1 in 5 U.S. adults over 75 remains edentulous. The prevalence typically rises in advanced old age because restorative treatments become more complicated, and chronic health issues can compromise oral care.
- Younger adults fare much better, with the majority (over 65%) in their 20s and 30s retaining all their permanent teeth. By contrast, only around one-third of adults over 40 have a full set of teeth, illustrating that middle age marks a shift in oral health status for many Americans.
- Globally, the same age gradient persists. In many high-income countries, older adults are keeping more of their teeth than ever, while in certain low-income regions, limited access to care causes high rates of tooth extraction in later life.
Gender Differences: A Shrinking Disparity
For many years, studies showed that women were slightly more likely to be edentulous than men, especially in older cohorts. Recent U.S. data, however, point to a near-equal prevalence:
- Equalizing Rates: Current national surveys find no statistically significant difference in the rate of complete tooth loss between older men and older women. This marks a considerable shift from earlier decades, when older women more frequently had lost all their teeth.
- Possible Explanations: Improvements in oral care access, preventive education, and dental technology benefit both genders. Women, who historically faced hormonal or pregnancy-related gum challenges, may be accessing better interventions today.
- Denture Use: While overall edentulism rates have leveled out, around 24% of women wear dentures (full or partial) compared to about 19% of men. Women’s longer life expectancy and desire for esthetic tooth replacements may help explain this small difference in prosthetic adoption.
Geographic Disparities in the United States and Beyond
Geographic location has an outsized effect on oral health, as access to fluoridated water, availability of dentists, and socioeconomic factors vary widely:
- U.S. Regional Patterns: The Southeast and parts of Appalachia show the highest edentulism rates among older adults, with some states reporting 16 to 26% prevalence of complete tooth loss. States in the Midwest and West, such as Utah, Illinois, and Wisconsin, tend to report lower rates (6 to 11%).
- Rural vs. Urban: Over 57 million Americans live in areas designated as dental health professional shortages, and many of these regions are rural. People in rural areas are thus more likely to lose teeth due to insufficient preventive or restorative care.
- Global Context: On the global stage, edentulism rates can range from around 3% in countries like Ghana to 20% or more in parts of Latin America. In Asia, countries such as China (9%) and India (16%) also illustrate the variability tied to socioeconomic and healthcare factors. Developed nations with robust public health measures generally have lower edentulism and better tooth retention.
Socioeconomic Correlations with Tooth Loss
Perhaps the most striking data point is the strong relationship between socioeconomic status (SES) and the likelihood of losing teeth:
- Income and Education Gaps: Among older adults in the lowest income brackets, complete tooth loss can exceed 30%, whereas it dips to below 12% for higher-income groups. Similarly, adults with less than a high school education have roughly triple the rate of edentulism compared to those with more formal schooling.
- Insurance Coverage: People with consistent dental insurance (private or through comprehensive public programs) are more likely to receive preventive treatments, fillings, and gum therapy before problems escalate to extractions. In contrast, adults without coverage often resort to emergency treatments like extractions when the pain becomes unbearable.
- Smoking and Oral Health: Smoking remains more prevalent in lower-income populations, compounding risks of severe gum disease and eventual tooth loss. In one national estimate, edentulism among older smokers reached 29%, compared to 12% for non-smokers.
- Cycle of Disadvantage: Missing teeth can hinder employability, further restricting income and perpetuating the inability to afford proper dental care. This cycle underscores the need for broad policy interventions to reduce oral health inequities.
Prevention Strategies Yield Results
One of the clearest findings in the research is that prevention works. The downward trend in edentulism over the past few decades can be credited to:
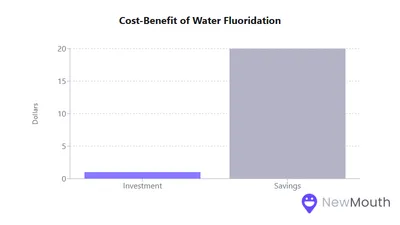
- Water Fluoridation: Community water fluoridation lowers cavities by roughly 25% in both children and adults. This translates to fewer extractions, as teeth remain healthier from the start.
- Regular Dental Visits and Hygiene: Check-ups catch issues like decay or gum disease early. Filling a cavity or treating mild gum disease is vastly cheaper than an extraction-and-replacement scenario later.
- Tobacco Cessation: Smoking doubles or even triples the odds of tooth loss due to periodontal damage. Public health campaigns to reduce smoking have a direct spillover benefit to oral health.
- Early and Ongoing Education: Promoting daily brushing, flossing, and healthy diets at the school level fosters a culture of preventive care. Dental sealants and fluoride varnishes are also used extensively to protect children’s teeth, helping ensure that adults keep more of their natural dentition.
Treatment Choices for Missing Teeth
When prevention arrives too late and a tooth is lost, people generally opt for one of three solutions: removable dentures, fixed bridges, or dental implants (including implant-supported restorations). Adoption rates vary based on cost, personal preference, and clinical suitability:
- Removable Dentures: Still the most common option, especially for multiple missing teeth or full arches. They are relatively low-cost compared to implants. However, they may require adhesives and periodic replacements.
- Fixed Bridges: These involve crowning adjacent teeth to support a false tooth. Bridges are popular among those who want a non-removable solution but cannot afford or do not qualify for implant surgery.
- Dental Implants: The fastest-growing tooth replacement option, offering a near-natural look and function. Roughly 6% of Americans currently have at least one dental implant, which is still a small minority, but a significant increase compared to 20 years ago. Cost remains the biggest barrier, with single implants often totaling several thousand dollars.
- Implant-Supported Dentures: A middle ground between conventional dentures and full fixed implant bridges. Removable prosthetics “snap” onto two to four implants, offering better stability but at a higher expense than a standard denture.
Quality of Life Effects
Teeth are vital for more than just chewing. Their presence or absence shapes a person’s daily experiences:
- Diet and Nutrition: Missing teeth or poorly fitting dentures cause people to avoid hard, fibrous foods. This dietary limitation can lead to reduced intake of fruits, vegetables, and proteins, risking malnutrition or an unhealthy reliance on softer refined carbohydrates.
- Speech and Social Comfort: Even a single missing front tooth can alter speech sounds. With multiple lost teeth, people often grow self-conscious, smile less, and may retreat from social situations to avoid embarrassment.
- Self-Esteem and Mental Health: Individuals with extensive tooth loss report feeling older, less confident, and sometimes depressed. The social stigma surrounding missing teeth compounds these emotional burdens.
- Functional Limitations: Struggles with chewing or speaking can create practical hurdles at work and in social settings, limiting a person’s opportunities or willingness to engage.
Tooth Loss and Nutrition: A Reciprocal Relationship
Tooth loss and poor nutrition can form a feedback loop:
- Chewing Difficulty → Poor Diet: Lower chewing efficiency often leads to eating soft, processed foods and reduced nutrient intake. Over time, insufficient vitamins, minerals, and protein may worsen overall health, which in turn negatively affects oral tissues.
- Micronutrient Deficiencies: Older edentulous individuals commonly have lower intakes of Vitamin C, fiber, and iron due to limited fruit, vegetable, and lean meat consumption.
- Malnutrition and Frailty: For seniors, compromised diets can accelerate frailty, weakening muscles and bones. This frailty can limit mobility and complicate dental visits, perpetuating the cycle of oral neglect.
Patient Preferences for Tooth Replacement
Studies consistently find that, in an ideal world, most patients prefer fixed, stable solutions over removable appliances:
- Natural Feel: Implants and fixed bridges are valued for their near-natural chewing force and appearance. Many denture wearers express dissatisfaction with stability despite lower costs.
- Aesthetics and Confidence: Particularly for front-tooth replacements, people strongly favor options that look indistinguishable from real teeth.
- Cost Constraints: Despite a clear preference for implants, only around 26% of edentulous patients in one study seriously considered implant therapy, primarily because implants are expensive and often not fully covered by insurance.
- Cultural Normalization: In communities where denture use is common, some patients remain content with removable options. Others, especially younger adults, increasingly see dentures as a last resort.
Financial Burden of Tooth Loss and Its Treatment
Tooth loss can be financially taxing, whether paying for replacements or incurring indirect costs:
- High Treatment Costs: A basic full denture might cost $1,000 to $3,000, whereas an implant-supported full-arch solution can run $20,000 to $45,000 per arch. Even single-tooth implants frequently exceed $3,000 each.
- Insurance Gaps: Most U.S. dental plans have low annual caps, and Medicare does not typically cover routine dental care for seniors. As a result, many retirees cannot afford ideal replacements.
- Preventive Savings: In contrast, preventive measures, like check-ups, cleanings, and fluoride treatments, are far cheaper than tooth replacement. Public health data repeatedly show that every dollar invested in fluoridation or early intervention returns multiple dollars in avoided treatment costs.
- Hidden Economic Costs: Productivity losses, job discrimination, and social stigma around missing teeth add intangible but significant costs to individuals and communities.
Influence of Insurance on Access to Care
Insurance coverage stands out as one of the strongest predictors of tooth retention:
- No Coverage, More Extractions: An estimated 68 million adults in the U.S. have no dental insurance, often resorting to emergency room visits that lead to tooth extractions instead of restorative care.
- Medicaid Limitations: Adult dental coverage under Medicaid varies widely by state. In states covering only “emergency” dental services, extraction is typically reimbursed, but not preventative fillings or dentures, leading to higher tooth loss rates.
- Employer-Sponsored Plans: Those with comprehensive private dental insurance are more likely to receive preventive treatments and thus face fewer extractions. However, even good plans may partially or fully exclude dental implants, steering patients toward bridges or dentures.
Maintenance Behaviors Across Demographics
The day-to-day habits of brushing, flossing, and regular dentist visits significantly shape who ends up losing teeth:
- Age Challenges: Younger adults benefit from better prevention messaging in schools, but they may skip professional care once they transition off parental insurance. Seniors, meanwhile, deal with dexterity issues or assume tooth loss is inevitable.
- Gender Differences: Women tend to brush and floss more consistently, though historically, they faced higher edentulism. With improved care, the sex-based gap in tooth loss has largely closed.
- Rural vs. Urban: Rural communities generally have fewer dentists, less fluoridated water, and cultural norms that accept tooth pulling as standard. Urban populations often have greater access to preventive services and advanced treatments.
Links Between Tooth Loss and Systemic Health
Mounting evidence demonstrates that the mouth is intricately connected to overall health:
- Cardiovascular Disease: Chronic inflammation from gum disease, often the precursor to tooth loss, has been associated with increased risk of heart attack and stroke. Periodontal disease affects more adults than many realize.
- Diabetes: People with poorly controlled diabetes experience more severe periodontal disease, leading to higher rates of extractions. In turn, tooth loss complicates nutrition management for diabetics.
- Respiratory Health: Nursing home residents with poor oral health are at higher risk of aspiration pneumonia. Simply improving oral hygiene can reduce lung infections.
- Mortality Risk: Studies link complete tooth loss with a higher risk of early mortality. While tooth loss itself may not directly cause death, it often signals underlying medical and nutritional challenges.
Social Implications of Missing Teeth
Oral health affects not only physical well-being but also social standing:
- Confidence and Self-Esteem: Gaps in one’s smile can lead to embarrassment, diminished self-confidence, and avoidance of social gatherings.
- Stigma and Employability: Employers may perceive missing teeth as unprofessional, and individuals with visible dental issues sometimes face hiring discrimination. This reinforces socioeconomic disparities.
- Psychological Toll: Many people with extensive tooth loss report feeling isolated or depressed. They may opt out of public events or personal relationships, worried about how others will judge their appearance.
Long-Term Outcomes and Future Projections
Tooth loss can have enduring consequences if not addressed:
- Bone Resorption: After tooth removal, the jawbone in that area gradually shrinks, potentially causing changes in facial structure and the fit of any denture.
- Repeated Costs: Dentures often need replacement every 5 to 10 years. Bridges may fail if the supporting teeth decay. Implants can last decades but require ongoing hygiene to avoid peri-implant disease.
- Population Trends: Although edentulism rates at a given age are falling, global aging means the absolute number of older adults with missing teeth will keep climbing. By 2050, estimates suggest over 600 million people worldwide could be completely edentulous.
- Optimistic Trajectory: Public health goals emphasize reducing tooth loss through water fluoridation, better access to preventive care, and expanded insurance coverage. Continued improvements in dental technology, such as more affordable implants, may also accelerate declines in edentulism.
The data show encouraging signs of progress over the past decade. However, large segments of the population, especially low-income and rural Americans, still face high rates of tooth extraction and limited replacement options. These statistics highlight one central insight: tooth loss seldom occurs in isolation. It is interwoven with economic status, chronic diseases, public policy, and societal attitudes.
Looking ahead, policymakers, dental professionals, and communities can leverage this deep pool of research to continue lowering tooth loss rates. By expanding coverage, intensifying preventive measures, and ensuring that quality care is accessible, we can help more people avoid the physical, financial, and emotional burdens of tooth loss.
Ultimately, the numbers paint a hopeful but nuanced portrait: tooth loss is far less common than it once was, yet it remains a serious public health challenge with profound personal and societal costs. Maintaining a strong focus on prevention, coupled with comprehensive approaches to care, can ensure that future generations keep their smiles healthier and longer than ever before.
Above all, the numbers show that tooth loss is largely preventable. Continued research and targeted interventions can ensure that the impressive improvements in tooth retention seen over the last few decades become the norm rather than the exception, bringing us closer to a future in which losing teeth prematurely is no longer a routine part of aging.
Sources
- AARP – https://www.aarp.org/health/healthy-living/info-2024/replacing-missing-teeth.html
- American College of Prosthodontists (ACP) – https://www.gotoapro.org/facts-figures/#:~:text=About%2023%20million%20are%20completely,and%20some%20forms%20of%20cancer
- Biltmore Periodontics – https://www.biltmoreperiodontics.com/oral-health-tooth-loss-within-americas-aging-population/#:~:text=Overall%2C%2017,today
- CareQuest Institute for Oral Health – https://www.carequest.org/about/press-release/new-report-685-million-adults-us-dont-have-dental-insurance-may-rise-914
- Centers for Disease Control and Prevention (CDC) – https://www.cdc.gov/cdi/indicator-definitions/oral-health.html
- Centers for Disease Control and Prevention (CDC) – https://www.cdc.gov/fluoridation/about/statement-on-the-evidence-supporting-the-safety-and-effectiveness-of-community-water-fluoridation.html
- Centers for Disease Control and Prevention (CDC) – https://www.cdc.gov/nchs/products/databriefs/db197.htm
- Centers for Disease Control and Prevention (CDC) – https://www.cdc.gov/nchs/products/databriefs/db368.htm
- Centers for Disease Control and Prevention (CDC) – https://www.cdc.gov/oral-health/about/about-tooth-loss.html
- Centers for Disease Control and Prevention (CDC) – https://www.cdc.gov/oral-health/health-equity/index.html
- Centers for Disease Control and Prevention (CDC) – https://www.cdc.gov/oral-health/php/2024-oral-health-surveillance-report/selected-findings.html
- Dental Disparities among Low-Income American Adults: A Social Work Perspective - PMC – https://pmc.ncbi.nlm.nih.gov/articles/PMC4985883/#:~:text=Not%20only%20does%20poor%20oral
- Dentures Statistics 2025-2024: Essential Stats w/ Facts & Data – https://impressionsdental.com/blog/dentures-statistics-2024/#:~:text=Around%2042
- John P. Goodman DDS – https://www.johngoodmandds.net/services/dental-implants/cost/#:~:text=Dental%20Implants%20Cost%20Kansas%20City%2C,can%20cost%20%2420%2C000%20to%20%2445%2C000
- Nascimento et al., Burden of Severe Periodontitis and Edentulism (PubMed) – https://pubmed.ncbi.nlm.nih.gov/39192495/#:~:text=Results%3A%20%20In%202021%2C%20over
- National Association of Dental Plans (NADP) – https://www.nadp.org/about-dental-plans-care/understanding-dental-benefits/#:~:text=Who%20has%20dental%20benefits%20today%3F
- Patel, The Epidemiology of Edentulism and Associated Factors (PMC) – https://pmc.ncbi.nlm.nih.gov/articles/PMC7346915/#:~:text=The%20epidemiology%20of%20edentulism
- Sociodemographic Factors and Implant Consideration by Patients Attending Removable Prosthodontics Clinics - PMC – https://pmc.ncbi.nlm.nih.gov/articles/PMC9293525/#:~:text=Treatment%20options%20presented%20by%20dental

Seasoned health writer translating complex dental topics into reader-friendly content.
Related Articles
The Power of Fluoridation: Statistics on Improved Oral Health
Water fluoridation remains one of the most studied and widely implemented public health initiatives aimed at reducing de...

A Guide to Treating and Preventing Gum Inflammation
Gum inflammation, or gingivitis, is a condition characterized by red, swollen, and irritated gums. It's often a precurso...

Dental Fluorosis: Causes, Symptoms & Treatment
This article offers you a complete guide to dental fluorosis. Read on to learn more about this condition, its causes, pr...

The Effects of Anxiety and Depression on Oral Health
What are the effects of anxiety and depression on oral health? Read on to find out and learn some oral health tips for p...