What Are Dental Health Differences in Rural vs. Urban Areas?
Reader-supported. We may earn a commission from links on this page. Advertising disclosure.
In this article
Dental health in the United States varies significantly by location, and the divide between rural and urban areas remains a pressing concern. Many rural communities face persistent challenges (fewer dentists, lower insurance coverage, and limited preventive programs), contributing to disparities that carry long-term health consequences.
Here we examine the core statistical data behind these differences. We look at provider availability, cost variation, barriers to care, insurance coverage trends, and oral health outcomes to illuminate how geography shapes dental care access and treatment.
These data-driven insights underscore the extent of the rural-urban gap and highlight strategies that public health initiatives have taken to address it.
Noteworthy Statistics
- Significant Dentist Shortages in Rural Areas: Rural communities have about 25 to 30 dentists per 100,000 people, whereas urban areas average 60 to 70 dentists per 100,000.
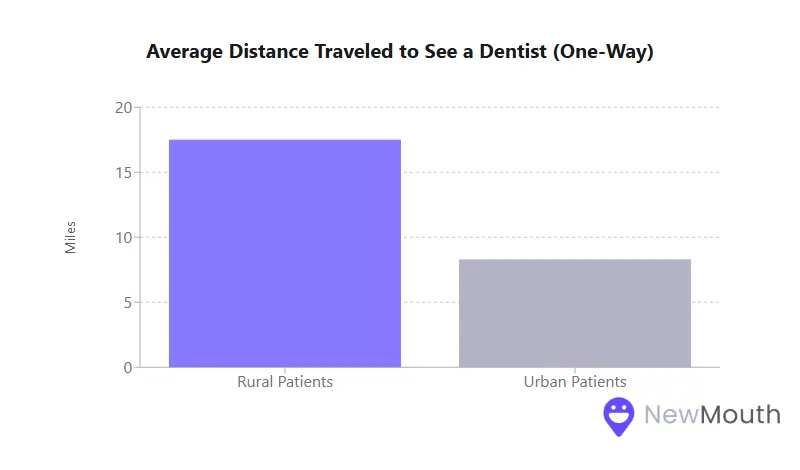
- Distance and Travel Burdens: Rural patients travel nearly twice as far to see a dentist (about 17.5 miles one way) compared to urban patients (8.3 miles).
- Fewer Preventive Visits: Around 40% of rural adults had not seen a dentist in over a year, compared to 30% in suburban or urban areas.
- High Rates of Tooth Loss: Rural adults are nearly twice as likely to have lost all their natural teeth by late middle age compared to their urban counterparts.
Provider Availability and Workforce Distribution
Provider availability is a foundational metric for understanding disparities in dental health. When communities lack an adequate supply of dentists, residents naturally face fewer options for preventive and restorative care.
- Dentist-to-Population Ratios
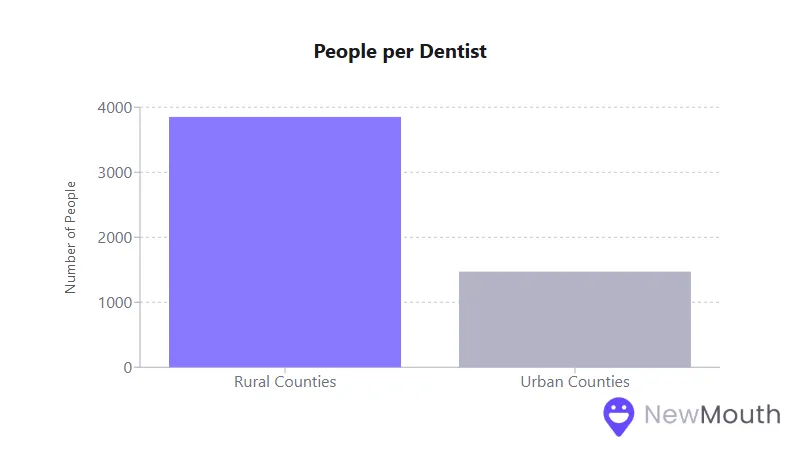
- Rural counties average only about one dentist per 3,850 people, whereas urban counties have one per 1,470.
- The overwhelming majority of dental specialists (endodontists, periodontists, pediatric dentists) practice in urban areas, leaving many rural regions without local specialists.
- Dental Health Professional Shortage Areas (HPSAs)
- Approximately two-thirds of designated Dental HPSAs are in rural areas, reflecting persistent recruitment and retention challenges.
- Many rural counties have no dentist willing to accept public insurance, further restricting access.
- Aging Rural Workforce
- Rural dentists tend to be older on average. Many plan to retire in the coming years, and replacing them is difficult.
- Despite overall growth in the number of dentists nationwide, rural dentist counts are often flat or declining.
These workforce gaps directly shape patients’ ability to receive consistent dental care. Without stable access to local providers, residents must either travel long distances or forgo care entirely.
Cost Variation: Routine vs. Major Procedures
Understanding how procedure costs differ between rural and urban settings reveals both nominal and relative affordability challenges.
- Routine Care Fees
- Routine cleanings and exams may cost slightly less in small-town practices, largely due to lower overhead. However, rural incomes also tend to be lower, so even reduced fees can be a steep expense.
- In urban markets, overhead costs are higher; a simple cleaning can reach the upper end of national price ranges.
- Major Treatments
- Root canals, crowns, implants, and orthodontic work are typically more expensive in cities but are also more widely available.
- Rural patients might save marginally on procedure fees but face additional travel costs and may have difficulty accessing specialists who perform advanced treatments.
- Insurance Reimbursement
- Public insurance (like Medicaid) reimbursement rates are frequently lower in rural areas, discouraging some dentists from practicing there.
- Private insurance coverage is less common among rural workers, compounding the cost burden when major dental work is needed.
While nominal prices can be lower in rural offices, the overall financial impact on households may be greater. For many rural families, high out-of-pocket costs remain a key reason for delaying or avoiding needed dental procedures.
Key Access Barriers
Barriers to care have a profound effect on dental health outcomes. Identifying these obstacles helps explain why rural communities exhibit higher rates of untreated decay and tooth loss.
- Geographic Isolation and Transportation
- With few or no public transit options in rural areas, patients who lack reliable personal transportation are at a disadvantage.
- Travel distances of 20, 30, or more miles each way for basic dental visits are not uncommon, discouraging regular check-ups.
- Insurance Gaps
- Rural residents are less likely to have employer-sponsored dental coverage.
- Although rural populations rely more on Medicaid, adult dental benefits under Medicaid may be minimal or nonexistent in some states.
- Financial Constraints
- Poverty levels are higher in rural America, and many jobs do not provide dental benefits.
- Even modest out-of-pocket costs can prove prohibitive, leading to delayed or incomplete treatment.
- Health Literacy and Cultural Norms
- Some rural communities have lower oral health literacy, contributing to less frequent preventive care.
- Cultural attitudes that accept tooth loss as “inevitable” can reduce the sense of urgency for seeking treatment.
Addressing these barriers, particularly transportation, affordability, and insurance coverage, remains essential for narrowing the rural-urban gap in oral health.
Insurance Coverage Discrepancies
Insurance coverage underpins much of the rural-urban disparity in dental care utilization. People with robust coverage are more likely to seek regular preventive services.
- Lower Dental Insurance Rates
- A higher percentage of rural adults lack dental insurance altogether (over one-third in many surveys) versus roughly one-quarter in urban areas.
- For children, rural households depend heavily on Medicaid or CHIP, yet acceptance by dental providers can be spotty.
- Private vs. Public Coverage
- Urban workers often benefit from employer-sponsored dental plans. Meanwhile, small businesses or farming operations rarely offer such benefits.
- Adult Medicaid benefits vary widely by state. Many states with large rural populations offer only limited or emergency dental coverage for adults.
- Provider Acceptance
- Among dentists nationwide, less than half accept Medicaid or CHIP patients. In some rural regions, not a single local practice will see publicly insured adults.
- Even if a rural family has Medicaid, they may have to travel to an urban area to find a participating dentist.
In essence, the insurance gap drives down preventive visits and early intervention in rural areas. Strengthening coverage both in scope and acceptance could significantly improve rural dental outcomes.
## Emergency Department Usage
When people cannot access routine dental services, they often resort to hospital emergency departments (ERs) for urgent oral health crises.
- Rural ER Visit Rates
- Rural residents experience more than double the rate of dental-related ER visits compared to those in large metropolitan areas.
- Typical ER visits involve severe tooth pain or infections that could have been prevented with earlier intervention.
- High Costs, Limited Solutions
- ERs are rarely equipped to provide definitive dental treatment. Patients may only receive antibiotics and pain relief.
- Repeated ER visits add up for state Medicaid programs and hospitals. Without follow-up care, the same issues can recur, escalating overall costs.
- Contributing Factors
- Severe provider shortages, long travel distances, and limited insurance acceptance leave some patients with no other option.
- The lack of specialty services means even treatable conditions might escalate into emergencies if a rural dentist cannot perform complex procedures.
Reducing ER visits for dental issues requires expanding preventive care, improving clinic availability, and promoting earlier treatment across rural communities.
Preventive Program Reach
Preventive dentistry is vital for reducing cavities, gum disease, and costly procedures later on. However, the reach and effectiveness of preventive programs differ markedly by location.
- Water Fluoridation
- Most major cities fluoridate their water, reducing cavity rates significantly. Many rural areas rely on well water or small private systems that are not fluoridated.
- Adding fluoridation infrastructure can be expensive for small rural municipalities, limiting adoption.
- School-Based Services
- Urban schools often partner with local dentists or nonprofits to provide sealants, fluoride treatments, and check-ups.
- Rural schools do have mobile dental programs in some states, but coverage is frequently limited, leaving gaps where children never receive basic preventive care at school.
- Sealant Initiatives
- Dental sealants can prevent up to 80% of cavities in children’s molars. Rural-based programs exist but are less widespread, given workforce challenges and travel costs.
- Large-scale sealant programs in urban districts (backed by city health departments) tend to serve a higher percentage of at-risk youth.
Despite proven results, many rural communities lack consistent, long-term preventive strategies. Expanding these services, particularly water fluoridation and in-school dental clinics, represents one of the most cost-effective paths to improving rural oral health.
Transportation Challenges and Their Effects
Transportation is a hidden but powerful driver of dental care disparities. Rural residents frequently cite travel logistics as a central obstacle.
- Long Travel Distances
- In many rural counties, the distance to the nearest dentist can exceed 20 miles, more than double the typical urban distance.
- Harsh weather, rising fuel costs, and lack of reliable vehicles compound the difficulty of maintaining regular check-ups.
- Limited or No Public Transit
- In contrast to most cities, rural areas rarely have bus lines or ride-share services for medical appointments.
- Some communities rely on volunteer shuttles or mobile dental vans, but such services are sporadic.
- Impact on Utilization
- Patients may consolidate multiple treatments into one visit, or they may forgo treatment altogether.
- Delays in care often mean more extensive interventions are needed later, leading to higher costs and worse outcomes.
Mitigating the travel barrier might involve expanding mobile clinics, offering free or low-cost transportation, or providing teledentistry to screen patients remotely and reduce unnecessary trips.
Technology Adoption (Teledentistry and More)
Dental technology can streamline care, improve diagnosis, and reduce time in the chair. While urban clinics lead in adopting advanced tools, rural areas have begun to embrace certain innovations out of necessity.
- Teledentistry
- Telehealth usage for dental consultations increased during the pandemic, especially in isolated communities.
- Rural patients stand to benefit from remote exams to determine if in-person appointments are needed, saving them long drives.
- Digital Imaging and Software
- Larger urban clinics often have the latest digital X-ray systems, 3D scanners, and AI diagnostic tools.
- Many solo rural practices still rely on older equipment due to cost and the difficulty of securing technical support.
- Broadband Constraints
- Robust internet access is crucial for uploading digital scans or video conferencing with specialists, which can be challenging in remote areas.
- Investments in rural broadband could accelerate telehealth adoption, making advanced dental care more accessible.
While full-scale technology deployment is more common in cities, targeted teledentistry initiatives show promise in bridging rural service gaps, particularly for screening and specialist referrals.
Treatment Plan Completion Rates
Even if an individual sees a dentist and receives a recommended treatment plan, completing that plan can be a challenge, particularly in rural regions.
- Cost and Insurance Hurdles
- Rural patients frequently cannot afford multiple appointments or out-of-pocket expenses for advanced procedures.
- The high prevalence of uninsured or publicly insured individuals reduces the likelihood of following through on multi-step treatments.
- Logistical Difficulties
- Long drives for each appointment make multi-visit treatments like root canals and crowns particularly burdensome.
- Some patients opt for extractions over restorations, knowing they cannot return for repeated appointments.
- Specialist Referrals
- Urban patients typically have local endodontists or oral surgeons, making referrals easy.
- Rural patients referred to a distant specialist often forgo that care due to cost or travel complications.
The net result is higher rates of incomplete or postponed treatments, which can worsen oral health and lead to preventable tooth loss over time.
Quality of Care Metrics
When people do receive dental care, rural-urban differences in the technical quality of care are not necessarily stark. Dentists nationwide hold similar credentials. However, the context in which rural dentistry occurs can affect outcomes.
- Provider Training and Scope
- Rural dentists sometimes handle more complex cases themselves due to a lack of specialists, and many are adept “generalists.”
- Urban dentists can refer out difficult procedures, potentially improving outcomes for complex needs.
- Advanced Equipment and Facilities
- Some rural clinics use older technology or have minimal staff.
- Urban facilities, especially corporate or group practices, often upgrade equipment frequently, enabling certain procedures to be faster and more precise.
- Outcome Differences
- Rural adults have higher rates of extractions, indicating that issues may be more advanced by the time of diagnosis.
- In many cases, “quality of care” for a single procedure may be on par with urban standards; the broader environment (lack of preventive visits and limited follow-up) creates worse overall outcomes.
Thus, individual dentists’ skills may be comparable, but the systemic constraints in rural settings lead to lower success rates in saving teeth and preventing disease.
Patient Satisfaction Trends
How patients perceive their dental care is shaped by both personal interactions and the broader delivery system.
- Satisfaction with Personal Care
- Rural patients often report strong relationships with their local dentists. The personal attention of a small practice can foster loyalty.
- In some surveys, they express satisfaction with the friendliness of staff but dissatisfaction with other logistical hurdles.
- Satisfaction with Access and Costs
- Lower marks typically arise from appointment availability, cost, and limited treatment options in rural clinics.
- Urban patients can choose from numerous providers, potentially improving satisfaction with convenience, even if actual costs may be higher.
- Overall Rating of Oral Health
- In self-assessments, a larger share of rural adults rate their oral health as “fair” or “poor.”
- By contrast, more urban patients say they have “good” or “excellent” dental health, reflecting both actual outcomes and perceived accessibility.
Patient satisfaction is multifaceted: rural residents might praise the care they receive when they get it, yet remain frustrated by barriers and out-of-pocket expenses.
Disparities in Specialty Care
Access to specialized dental services (orthodontics, pediatric dentistry, periodontics, and oral surgery) is heavily skewed toward metropolitan areas.
- Rural Specialist “Deserts”
- Many rural counties do not have a local orthodontist or pediatric dentist, so families must often travel long distances for advanced treatments.
- Oral surgeons and endodontists generally cluster in high-population centers, leaving remote communities reliant on general dentists for complex procedures.
- Travel Burdens
- Specialist visits may require multiple appointments, compounding time off work and travel costs for rural patients.
- Some rural residents opt out entirely, choosing extraction or foregoing cosmetic and rehabilitative treatments.
- Tele-Specialty Consults
- Newer programs connect rural providers with distant specialists via teledentistry.
- This can guide care decisions but does not replace hands-on treatments like orthodontics or surgical interventions.
Unequal specialty availability further entrenches the rural-urban gap. For many, advanced dental care is simply out of reach unless they can bear the costs and logistics of traveling to a major city.
Public Health Initiatives and Their Impact
Government agencies and nonprofits have invested in multiple strategies to reduce oral health disparities. These programs have some successes but have not eliminated the rural-urban divide.
- Loan Repayment and Recruitment
- The National Health Service Corps and state-level initiatives offer student loan forgiveness to dentists who practice in underserved areas.
- While effective at placing some providers in rural clinics, retention after the commitment period is a constant challenge.
- Federally Qualified Health Centers (FQHCs)
- FQHCs deliver sliding-fee-scale dental services to low-income populations, serving as a safety net in many rural towns.
- Despite helping thousands of patients, these clinics often have waitlists and face staffing shortages, limiting overall capacity.
- Mobile and School-Based Clinics
- Nonprofits run free or low-cost dental events and send mobile units to rural schools.
- These programs address acute needs, especially for children, but are often sporadic rather than a year-round solution.
- Dental Therapy Legislation
- A few states authorize mid-level dental providers (dental therapists) to expand access in remote areas.
- Early results in places like Alaska show promise, with improved preventive care in isolated communities.
Public programs and nonprofit initiatives have unquestionably improved rural dental access. However, widespread and consistent coverage is needed to close the gap.
## Long-Term Oral Health Outcomes
Cumulative data reveal that rural Americans experience poorer oral health on average than their urban counterparts.
- Higher Tooth Loss
- By late middle age, rates of complete tooth loss (edentulism) are nearly twice as high in rural areas.
- Partial tooth loss is also more common, impacting chewing ability and overall quality of life.
- Untreated Decay
- A higher percentage of rural adults have untreated cavities, reflecting delayed or sporadic care.
- Rural children likewise have more caries, often linked to lower access to fluoride and fewer preventive services.
- Gum Disease and Oral Cancer
- Greater tobacco usage in rural regions correlates with heightened periodontal disease risk.
- Oral cancers tend to be diagnosed later, resulting in poorer survival rates compared to urban patients who undergo more regular screenings.
- Trends Over Time
- While overall national oral health has improved modestly in the last decade, rural gains lag behind, preserving or even widening the disparity.
- Addressing core issues (workforce distribution, insurance coverage, and preventive measures) remains crucial to altering these long-term patterns.
Ultimately, geographic location remains a potent determinant of oral health. Coordinated efforts to expand access in rural communities could significantly reduce these entrenched disparities.
Rural Americans face numerous disadvantages regarding dental health. These gaps are not superficial but accumulate into distinctly worse outcomes.
Despite many targeted interventions, the problem persists partly because it intersects with deeper issues like poverty, workforce shortages, and limited public infrastructure. The data suggest that boosting rural dental care will require sustained policy commitment, creative approaches (including teledentistry and mid-level providers), and expanded safety-net resources.
By prioritizing these efforts, stakeholders can move toward a future where one’s ZIP code no longer dictates the likelihood of maintaining a healthy smile. For policymakers, the evidence underscores the importance of comprehensive programs that blend financial incentives, preventive outreach, and infrastructure development.
With continued attention to statistical trends and proven interventions, the rural-urban dental divide can be diminished, and equitable oral health for all can be promoted.
Sources
- American Dental Association (ADA) – https://www.ada.org/en/science-research/health-policy-institute
- Business Wire – https://www.businesswire.com/news/home/20240117022637/en/New-Report-Rural-Populations-Have-Worse-Oral-Health-Care-Access-Utilization-and-Outcomes-Compared-to-Urban-Areas
- Harvard Gazette – https://news.harvard.edu/gazette/story/2025/01/new-study-maps-the-dental-deserts-in-the-u-s
- Oral Health in Rural Communities (Rural Health Information Hub) – https://www.ruralhealthinfo.org/topics/oral-health
- U.S. Health Resources & Services Administration (HRSA) – https://data.hrsa.gov/topics/health-workforce/shortage-areas

Web content writer specializing in making dental research accessible to diverse audiences.
Related Articles
Dental Implants: Success Statistics & Info for Replacing Missing Teeth
Dental implants are a transformative option for replacing missing teeth, commonly praised for their durability and natur...

Dental Surgery Recovery: Tips for Pain and Swelling Relief
Dental surgery, while often necessary for oral health, can cause discomfort in the form of pain and swelling. This is a...
How Does Dental Anxiety Affect Your Oral Health?
Dental anxiety (everything from mild nervousness to severe dental phobia) affects a significant portion of the populatio...

Can I Use Miswak Sticks to Clean My Teeth?
Miswak is a natural tool used for centuries to clean teeth. It's derived from the Salvadora persica tree (often referred...