Current State of Children's Oral Health in the US
Reader-supported. We may earn a commission from links on this page. Advertising disclosure.
In this article
Over the last decade, pediatric dental health in the United States has steadily improved in certain areas, yet persistent disparities and challenges remain. Tooth decay (dental caries) remains the most common chronic childhood disease, outpacing other conditions like asthma.
In response, numerous prevention programs, insurance expansions, and community initiatives have aimed to reduce untreated decay and improve access to care.
Public health data from 2015 through 2025 show shifts in cavity prevalence, treatment rates, and the cost-effectiveness of preventive care.
This article reviews the most relevant statistics on pediatric dental health in the U.S., including demographic patterns, school-based programs, and the financial trade-offs between prevention and treatment.
Noteworthy Statistics
- Cavity Prevalence in Preschoolers: An estimated 23% of U.S. children ages 2 to 5 have experienced dental caries in their baby (primary) teeth.
- Sealant Effectiveness: School-based dental sealant programs can lead to up to a 60% reduction in new cavities on sealed molars.
- Fluoridation ROI: For every $1 spent on community water fluoridation, between $8 to $49 is saved in avoided dental treatment costs.
- Delayed Treatment Consequences: Over 200,000 pediatric emergency department visits per year are due to preventable dental conditions, most commonly untreated decay.
Age-Specific Cavity Rates
Understanding cavity prevalence by age group is critical for targeting preventive interventions effectively. Data from national surveys over the past decade show distinct patterns of caries experience in different childhood stages:
- Preschool-aged (2 to 5 years)
- Approximately 23% of children in this age range have had decay in their primary teeth.
- In low-income preschoolers, untreated decay rates dropped from around 31% to 18% between the early 2000s and the mid-2010s, reflecting recent improvements in early dental intervention.
- Young Children (6 to 8 years)
- By age 8, over half of U.S. children have experienced at least one cavity in their baby teeth.
- Untreated decay in primary teeth hovers around 20% for this group. Children see a rapid rise in cavities once permanent teeth begin to erupt, reinforcing the importance of preventive measures like sealants and fluoride.
- Preteens (6 to 11 years overall)
- Roughly 21% have had caries in their permanent teeth.
- Sealant usage in this age group has climbed to over 40% in some states, aligning with a corresponding decline in the incidence of new cavities.
- Adolescents (12 to 19 years)
- Around 59% of teens have experienced at least one cavity in permanent teeth, increasing to roughly two-thirds by late adolescence.
- Untreated decay affects about 15% of adolescents, a statistic that has remained relatively unchanged for the last 10 to 15 years.
Demographic Disparities
Despite modest improvements in some age brackets, disparities persist. Children from minority backgrounds and those in low-income households continue to experience higher decay rates than their non-Hispanic White or more affluent peers.
Such gaps underscore the need for targeted interventions and expanded access to preventive care in underserved communities.
Prevention Program Effectiveness
Preventive measures have proven to be among the most significant factors driving positive shifts in pediatric oral health outcomes. These measures aim to halt decay before it begins or to detect and treat it in its earliest stages.
- Community Water Fluoridation
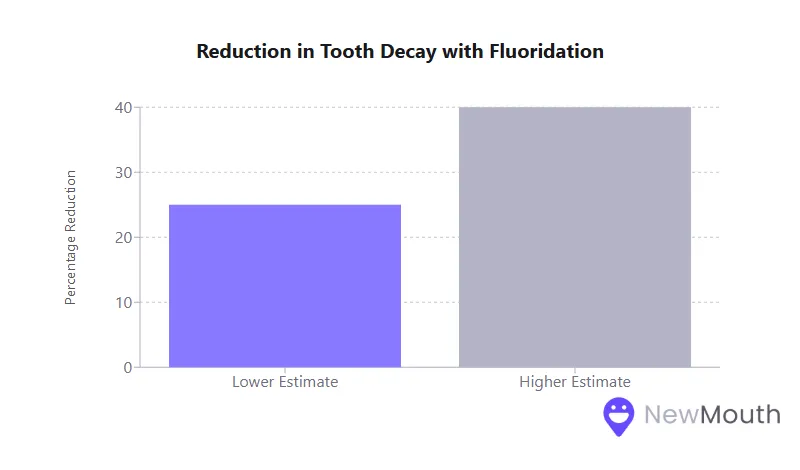
- Studies show a consistent 25 to 40% reduction in childhood tooth decay in optimally fluoridated communities, highlighting fluoridation’s lasting contribution to declines in caries.
- School-Based Dental Programs
- Bringing sealants, fluoride varnish, and screenings into schools can cut new cavities by up to 60% in participating children.
- Statewide expansions of school sealant programs helped boost sealant usage among low-income children by approximately 75% over the last 15 years.
- Fluoride Varnish and Clinical Prevention
- Routine fluoride varnish applications can reduce the development of cavities in primary teeth by 37 to 43% and remain an especially effective prevention strategy for high-risk toddlers.
- Community and Volunteer Initiatives
- Programs like free “Give Kids a Smile” days and local public health clinics have further broadened access to preventive services.
- These programs contribute to higher rates of dental visits: as of recent data, over 85% of children 2 to 17 years old have had a check-up in the past year.
Treatment Completion Rates
Even with a solid preventive infrastructure, many children who are diagnosed with dental issues never complete their full treatment plans, often due to logistical or behavioral barriers.
- Complex Treatment Plans: Multiple fillings or more extensive restorative procedures require additional appointments, which can deter families with limited time or resources.
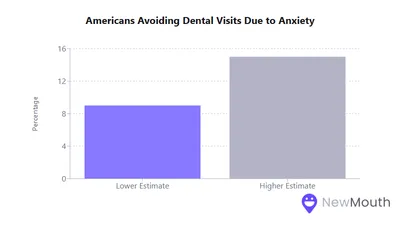
- Child Behavior and Anxiety: Uncooperative or fearful children may postpone or forgo recommended treatments, although sedation dentistry or hospital-based care can improve completion rates.
- Follow-Up Challenges: Referrals to specialists are commonly underutilized; in certain studies, as few as 15% of children referred for complex procedures ever received the needed treatment.
- Parental Factors: Caregivers’ dental literacy, anxiety, and availability significantly influence whether children complete all prescribed dental work.
Treatment completion tends to be highest when care is consolidated (e.g., performed under sedation in one session) and when parents receive strong support with scheduling, transportation, and overall guidance.
Sealant Usage Impact
Dental sealants, applied primarily to the grooves of children’s molars, are one of the most proven methods to halt cavity formation in hard-to-brush pits and fissures.
- High Efficacy: Sealants can prevent about 80% of cavities in the first two years after application, with protective benefits persisting for several years thereafter.
- Widespread Uptake: National data from mid- to late-2010s suggest 42% of children 6 to 11 and nearly half of the teenagers 12 to 19 have at least one sealed tooth.
- Key to Reducing Disparities: Low-income children who receive sealants in targeted programs see a marked reduction in new decay, partially closing the gap with higher-income peers.
Cost studies confirm that sealants are a cost-effective measure. They save money by preventing the need for more expensive restorative treatments.
School-Based Program Success
Schools represent a critical locus for delivering both preventive and routine oral health services to children, especially those who might otherwise face barriers.
- Cavity Reduction
- Comprehensive programs, offering sealants, fluoride applications, and cleanings, have cut new cavities in half in some populations.
- Even a single school-based intervention (e.g., a fluoride or sealant application) can prevent up to 80% of cavities in treated teeth.
- Improving Access and Equity
- School clinics eliminate cost and transportation barriers by providing care onsite, often at no out-of-pocket cost to families.
- These efforts are particularly beneficial in low-income or rural communities with significant provider shortages.
- Screening and Referrals
- School-based screenings identify urgent needs early.
- Follow-through on external referrals remains a challenge, though programs incorporating case management or tele-dentistry have demonstrated higher completion rates.
- Oral Health Education
- Classroom teaching and hands-on demonstrations (e.g., supervised toothbrushing) foster lifelong healthy habits, helping to drive down decay rates over time.
Fluoride Treatment Effectiveness
Fluoride, whether consumed through community water systems or applied topically, remains the cornerstone of preventing tooth decay in children:
- Community Fluoridation
- Associated with a 25 to 50% reduction in caries rates, making it one of the most effective large-scale public health measures.
- About 69% of Americans on community water systems benefit from fluoridation.
- Fluoride Varnish
- Applied 2 to 4 times per year, varnish lowers cavity risk by around 37 to 43% in primary teeth and around 40% in permanent teeth.
- Encouraged in medical settings, it has expanded significantly through pediatricians’ offices and public health programs.
- Fluoride Toothpaste and Rinse
- Brushing with fluoride toothpaste offers roughly 24% greater decay prevention than non-fluoride pastes, while supervised school-based mouth rinse programs yield an additional 20 to 30% reduction in permanent-tooth cavities.
Together, these fluoride-based strategies strengthen enamel against acid attacks and help reverse early-stage decay, lowering both immediate and long-term treatment costs.
Diet Correlation Patterns
Children’s dietary behaviors are tightly linked to their oral health outcomes. High sugar consumption, frequent snacking, and sugary beverages all contribute to cavity formation.
- Excess Sugar Intake
- The more added sugars a child consumes, the higher their risk of tooth decay.
- Sugar-sweetened beverages (SSBs) are the top source of added sugars for U.S. youth, with about two-thirds of children drinking at least one sugary beverage daily.
- Socioeconomic Links
- Food-insecure or low-income households may rely on cheaper, sugar-heavy foods, contributing to elevated cavity rates in these populations.
- Marketing and availability of sugary products also influence families across income levels.
- Recommended Limits
- Health organizations urge limiting added sugars to below 10% of daily calories (and ideally below 5%).
- Reducing sugary drink consumption is a key strategy to prevent caries, as constant sugar exposure fuels acid-producing bacteria that erode tooth enamel.
Oral Hygiene Habits
Daily brushing and flossing are foundational to oral health, yet surveys show significant room for improvement in children’s home care routines.
- Brushing Frequency
- Only about 64% of parents report their child brushes at least twice a day. A notable segment of children brush just once daily or less.
- Many parents struggle to enforce the recommended two-minute brushing guideline.
- Flossing Challenges
- Fewer than a quarter of children floss regularly. In some surveys, the majority of parents admit flossing occurs “less often than once a day” or is skipped entirely.
- Resistance to flossing and general lack of routine among children contribute to lingering plaque and higher cavity risk.
- Behavioral Hurdles
- Nearly half of parents find it more challenging to get kids to brush than to eat vegetables.
- However, families that set clear routines and supervise brushing through the early elementary years report fewer incidents of decay.
Childhood cavities correlate strongly with inconsistent oral hygiene. Improving these habits by age six or seven can greatly reduce ongoing decay into adolescence.
Parent Education Impact
Parental oral health literacy is a key determinant in whether children adopt good habits and receive early, consistent care:
- Education Level
- Children of parents with higher education levels tend to have fewer cavities, better access to preventive services, and more frequent dental visits.
- Health Literacy
- Parents aware of the need for early dental visits (by age one) and preventive care are more likely to have children with lower cavity rates.
- Families that understand the harm of sugary drinks and improper hygiene routines often enforce stricter oral health practices at home.
Low oral health literacy directly translates into higher rates of untreated decay and missed dental appointments. Consequently, many public programs now include caregiver education as a fundamental component of pediatric dental interventions.
Access Barrier Effects
Despite increasing insurance coverage and expanded public health measures, many children still face barriers that limit or delay their dental care:
- Cost Issues
- Families without insurance or with limited coverage often cite cost as the primary reason for postponing treatment.
- Even with Medicaid, locating a dental provider who accepts public insurance can be difficult.
- Provider Availability
- Only about one-third of dentists accept Medicaid in some regions, leaving many low-income children underserved.
- Rural areas and certain inner-city neighborhoods have persistent dentist shortages, forcing long travel or wait times.
- Transportation and Scheduling
- Parents who lack reliable transportation or flexible work schedules struggle to attend multiple appointments, particularly when children need restorative treatments.
- Vulnerable Populations
- Minority, low-income, and special-needs children face compounding barriers. They remain more likely to develop serious infections or require emergency department visits for preventable oral health issues.
Addressing these obstacles (e.g., through mobile clinics, teledentistry, or improved Medicaid reimbursement rates) is essential to ensure all children receive regular preventive services.
Insurance Coverage Impact
Dental insurance correlates strongly with a child’s likelihood of receiving timely care and maintaining good oral health.
- Coverage Expansion
- Policy reforms over the last decade have pushed pediatric dental coverage to around 90% of children, either through private plans or Medicaid/CHIP.
- As a result, the percentage of children with no annual dental visits has declined.
- Public vs. Private Plans
- Children with private insurance often have broader access to providers than those on Medicaid.
- Still, Medicaid-enrolled children fare better than uninsured children, emphasizing the importance of at least some form of coverage.
- Uninsured Children
- Those without dental insurance are at the highest risk for untreated decay.
- While the uninsured rate for children has fallen, specific subgroups, like undocumented immigrants, may lack coverage, compounding inequities.
Insurance coverage alone does not fully solve access problems. However, it remains a decisive factor in whether children see a dentist regularly and benefit from preventive interventions.
Emergency Visit Rates
Dental-related emergency department (ED) visits reveal the downstream consequences of untreated pediatric decay:
- ER Utilization
- Over 200,000 children per year visit emergency departments for non-traumatic dental conditions, primarily advanced infections from untreated cavities.
- Cost and Effectiveness
- These ER visits rarely resolve the underlying dental issue; patients typically receive pain relief or antibiotics and still require follow-up at a dental office.
- Most of these visits are publicly funded, creating a significant financial burden on Medicaid programs.
Although some regions report slight reductions in pediatric dental emergencies due to better prevention, they remain a costly symptom of delayed or inaccessible routine care.
Early Intervention Success
Establishing a dental home early and addressing problems in infancy or toddlerhood dramatically improves a child’s oral health trajectory:
- Age 1 Dental Visits
- When children begin routine checkups by their first birthday, they often need fewer fillings and have lower overall dental costs throughout childhood.
- Preventive vs. Restorative Pathways
- Early application of sealants or fluoride and swift treatment of small lesions prevent more extensive procedures like crowns or extractions.
- Long-Term Advantages
- Early intervention can slash the risk of severe early childhood caries, keep kids pain-free during crucial developmental years, and lay the foundation for lifelong healthy habits.
Communities emphasizing early dental visits combined with strong parent education have seen marked reductions in cavity rates among preschoolers.
Long-Term Outcome Metrics
The consequences of childhood oral health echo into adolescence and adulthood:
- Predictive Value of Early Caries
- Children with primary tooth decay are significantly more likely to develop decay in their permanent teeth.
- Tooth Retention in Adulthood
- Early and adequate care leads to higher rates of intact adult dentition, while chronic untreated childhood decay often results in tooth loss.
- Quality of Life
- Individuals with fewer negative dental experiences in childhood report lower dental anxiety and better overall oral health attitudes in adulthood.
Ensuring children remain cavity-free benefits them immediately and reduces their likelihood of major dental issues and associated costs well into their adult years.
Cost-Benefit Analysis: Preventive vs. Treatment Approaches
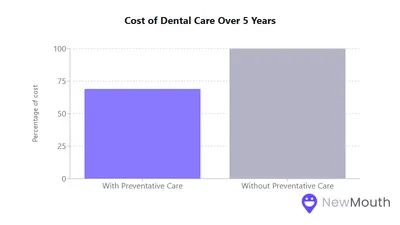
Economic analyses consistently reinforce that preventive care is far more cost-effective than expensive restorative or emergency procedures:
| Preventive Approach | Estimated Economic Benefit |
|---|---|
| Water Fluoridation | Every $1 invested saves $8 to $49 in treatment costs, translating to billions in total annual savings. |
| School Sealant Programs | Cost per sealant ($11 to $15) is significantly less than a filling ($50+), preventing major expenses. |
| Early First Dental Visit | Children starting dental checkups by age 1 incur around $300 less in treatment costs over five years. |
| Fluoride Varnish | Low material cost (~$1) with up to 40% cavity reduction in permanent teeth, avoiding high restorative fees. |
| Emergency/Delayed Care | A single pediatric ER visit can cost thousands and rarely solves the root problem, adding to long-term costs. |
By investing in fluoride, sealants, and early routine visits, communities and families can substantially lower both the prevalence of cavities and the financial burden of advanced treatments.
Pediatric dental health statistics highlight both encouraging progress in reducing early childhood caries and continuing barriers that limit access to and sustained care. The data suggest that sustained, preventive approaches can greatly reduce the pervasive burden of childhood tooth decay.
Over the years, improvements in insurance coverage and targeted prevention campaigns have helped increase the number of children receiving regular checkups and fluoride treatments. Yet disparities remain: families in underserved and rural areas, as well as special-needs children, continue to face significant challenges in obtaining care.
Statistics consistently show that these groups risk falling further behind without expanded school-based services and stronger safety-net programs. Looking ahead, policymakers and health professionals can build on the evidence that prevention pays off.
By amplifying preventive strategies, closing coverage gaps, and improving provider availability, communities can ensure that more children enjoy healthier smiles, avoid costly emergency treatments, and carry positive oral health behaviors into adulthood.
Sources
- American Academy of Family Physicians (AAFP) – https://www.aafp.org/pubs/afp/issues/2016/0501/p743.html
- American Dental Association (ADA) – https://www.ada.org/-/media/project/ada-organization/ada/ada-org/files/resources/research/dqa/dental-quality-measures/2024/2024_follow_up_after_ed.pdf
- Centers for Disease Control and Prevention (CDC) – https://www.cdc.gov/nchs/products/databriefs/db191.htm
- Centers for Disease Control and Prevention (CDC) – https://www.cdc.gov/oral-health/data-research/facts-stats/fast-facts-dental-sealants.html
- Centers for Disease Control and Prevention (CDC) – https://www.cdc.gov/school-health-conditions/chronic/oral-health.html
- Centers for Disease Control and Prevention (CDC) – https://www.cdc.gov/nchs/fastats/dental.htm
- Children’s Dental Health Disparities | The Pew Charitable Trusts – https://www.pewtrusts.org/en/research-and-analysis/articles/2016/02/16/childrens-dental-health-disparities
- Community-based Caries Prevention Strategies » Massachusetts Coalition for Oral Health – https://www.masscoalitionfororalhealth.org/program-planning-implementation/
- Delta Dental of Massachusetts Press Releases –Delta Dental Survey Says Parents Have Harder Time
- Forsyth Institute – https://forsyth.org/new-study-supports-the-effectiveness-of-the-forsythkids-school-based-dental-program-for-reducing-untreated-tooth-decay/
- KFF (Kaiser Family Foundation) – https://www.kff.org/medicaid/issue-brief/variation-in-use-of-dental-services-by-children-and-adults-enrolled-in-medicaid-or-chip/
- Michigan Medicine – https://www.michiganmedicine.org/health-lab/over-13-parents-say-their-child-has-experienced-dental-problems-reflect-oral-hygiene-habits
- National Institute of Dental and Craniofacial Research (NIDCR) – https://www.nidcr.nih.gov/research/data-statistics/dental-caries/children
- PubMed (National Library of Medicine) – https://pubmed.ncbi.nlm.nih.gov/28619207/
- Verywell Health – https://www.verywellhealth.com/school-based-dental-programs-access-5115983

Web content writer specializing in making dental research accessible to diverse audiences.
Related Articles

Best Foods for Healthy Teeth and Gums
What you eat plays a crucial role in maintaining a healthy mouth, and below we cover the best foods to incorporate into...

Best Natural Remedies for Treating Gum Disease
Having a good oral care routine is a great way to prevent gum disease and build the foundation for healthy gums. But the...
How Does Dental Anxiety Affect Your Oral Health?
Dental anxiety (everything from mild nervousness to severe dental phobia) affects a significant portion of the populatio...
Dental Care Spending: Statistics and Trends
Dental expenditures in the United States have steadily risen over the past decade, reflecting shifts in procedure costs,...