Herpangina: Symptoms, Causes, and How to Care for Your Child
Reader-supported. We may earn a commission from links on this page. Advertising disclosure.
In this article
Herpangina is a viral infection that causes painful blister-like sores in the back of the mouth and throat. It is caused by enteroviruses — most often coxsackievirus A — and most commonly affects children under 10, though older children, adolescents, and adults can also get it.15 Symptoms typically resolve in 7 to 10 days with rest, fluids, and pain relief.4 Serious complications are rare but possible in newborns, pregnant people, and people with weakened immune systems.
If you’re not sure which mouth condition your child has, our overview of toddler mouth sores compares the most common causes.
What Is Herpangina?
Herpangina is a common viral illness caused by enteroviruses, a family of viruses that includes many coxsackievirus strains as well as echoviruses and other types.15 It causes small blisters or shallow ulcers — each smaller than 5 mm across — on the soft palate, tonsils, uvula, and back of the throat. Children develop sores within 1 to 2 days of the fever starting.
The illness spreads easily in daycare centers and schools. Most children recover fully at home within a week.2
Herpangina Quick Facts
- What causes it? Enteroviruses — most often coxsackievirus A — are the main cause.15
- Is it contagious? Yes. It spreads through saliva, respiratory droplets, and stool, especially in daycare and school settings.39
- Is it the same as hand, foot, and mouth disease? No. The two are caused by related enteroviruses, but herpangina sores stay in the back of the mouth and throat. Hand, foot, and mouth disease (HFMD) also causes a rash on the hands, feet, and sometimes buttocks.3
- How long does it last? Most cases clear in 7 to 10 days. Mouth sores usually disappear within 1 to 7 days.24
Call your child’s doctor right away if your child:
- Has a stiff neck or severe headache
- Won’t drink fluids for 8 hours or more
- Shows signs of dehydration — no wet diaper for 8 hours, no tears when crying, dry mouth
- Has a rectal temperature of 100.4°F (38°C) or higher and is younger than 3 months old
- Has a seizure
- Has symptoms lasting more than 7 days
- Is a newborn, is immunocompromised, or you are pregnant and develop symptoms
See the full When to Call the Doctor section below for more detail.
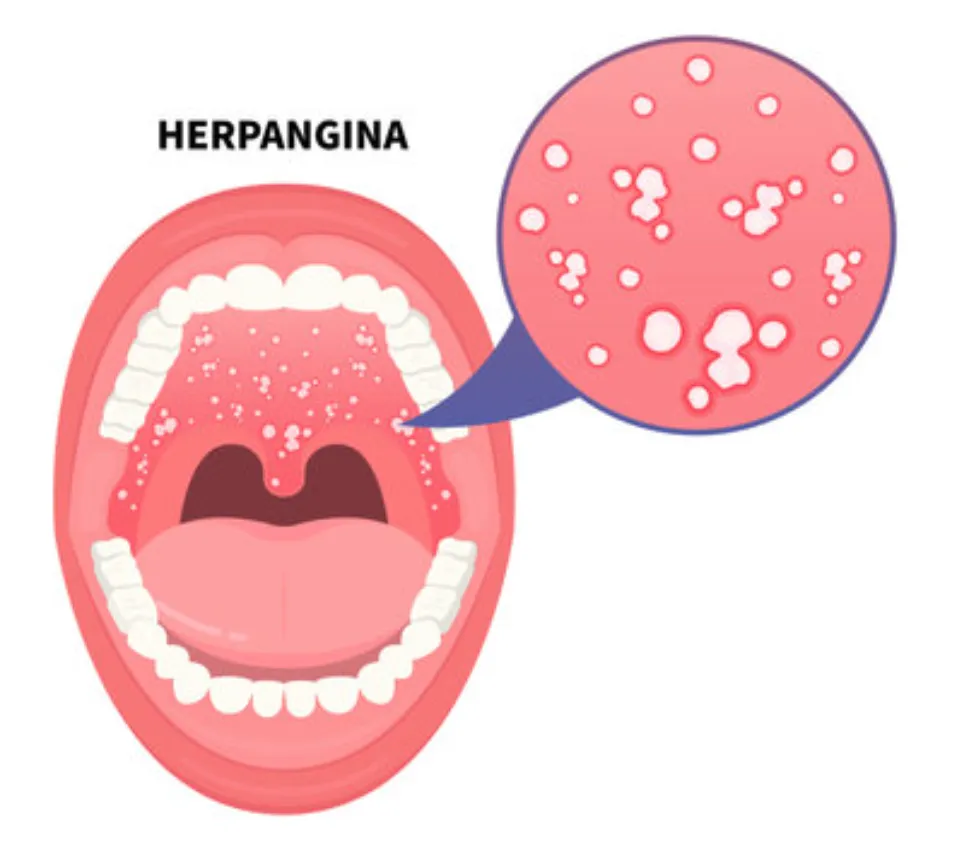
What Does Herpangina Look Like?
Herpangina sores appear in the back of the mouth — on the soft palate, tonsils, uvula, and posterior throat. They start as small grayish-white blisters and quickly become shallow ulcers with a red ring around them. Each sore is usually smaller than 5 mm across.110
The back-of-the-mouth location is what makes herpangina different from many other childhood mouth conditions. Cold sores form on the lips and look crusted. Canker sores appear on the inner cheeks and tongue, not the soft palate. Oral thrush shows up as white patches that wipe off, leaving red skin underneath — herpangina sores do not wipe off.10
Parents searching for what herpangina looks like sometimes mistake the sores for strep throat or tonsillitis. A key difference: strep throat rarely produces visible ulcers; it causes swollen tonsils with white patches or pus. A pediatrician can confirm the diagnosis with a quick physical exam.
Herpangina Symptoms in Children
Most children develop a high fever first, followed by mouth sores a day or two later. Symptoms appear within 3 to 5 days of exposure to the virus.1
Common symptoms include:
- High fever — Often the first sign, usually appearing before the mouth sores1
- Sore throat and difficulty swallowing — The back of the throat becomes swollen and painful
- Mouth sores — Grayish blister-like sores appear on the soft palate, tonsils, and uvula 1 to 2 days after the fever begins. They develop into shallow mouth ulcers within 24 hours12
- Refusing to eat or drink — Children avoid food and fluids because swallowing hurts
- Drooling — Younger children drool more because swallowing is painful
- Fussiness and tiredness — Babies and toddlers become irritable and harder to comfort
- Headache or body aches — More common in older children and adolescents
Symptoms last about a week. Mouth sores typically resolve within 1 to 7 days, and the fever passes in 2 to 4 days.410
Severe Symptoms in Children
Most herpangina is mild, but a small number of children develop more serious illness — usually when enterovirus 71 is the cause.1 Watch for:
- Neck stiffness
- Persistent severe headache
- Confusion or unusual sleepiness
- Trouble breathing
- Seizures
- Muscle weakness
These signs need urgent medical attention. See When to Call the Doctor for the full list.
What Causes Herpangina and How It Spreads
Herpangina is caused by enteroviruses, a family of common viruses. Coxsackievirus A is the most frequent cause, with coxsackievirus B and enterovirus 71 also responsible for many cases.1 Less common causes include echoviruses and other enteroviruses.15 Herpangina has no relation to herpes simplex infections — the name refers to the blister-like (“herpetic”) appearance of the sores, not to the herpes virus.5
How Herpangina Spreads
The viruses that cause herpangina spread easily, which is why outbreaks happen quickly in daycares, preschools, and schools. The main routes of transmission are:39
- Saliva and other mouth secretions
- Respiratory droplets from coughing, sneezing, or talking
- Stool (especially in diaper-age children)
- Direct contact with fluid from blisters
- Contact with surfaces or toys that have the virus on them
Humans are the only known carriers, but enteroviruses survive on surfaces for hours to days.9
Incubation and Contagious Period
The incubation period — the time between exposure and symptoms — is about 3 to 5 days.1 Children are most contagious during the first week of illness, when fever and sores are present. The virus can continue to shed for several weeks afterward, especially in stool, which is why thorough handwashing matters even after a child seems better.19
Herpangina vs. Hand, Foot, and Mouth Disease
The main difference: hand, foot, and mouth disease (HFMD) causes a rash on the hands and feet; herpangina sores stay in the mouth. Both are caused by overlapping enteroviruses, so the virus families and many symptoms look similar.3
| Feature | Herpangina | Hand, Foot, and Mouth Disease |
|---|---|---|
| Where sores appear | Back of the mouth: soft palate, tonsils, uvula, throat | Mouth, hands, feet, and sometimes buttocks or genitals |
| Body rash | Not typical — a rash on the hands, feet, buttocks, arms, or legs points to HFMD or a related enterovirus illness3 | Red spots or blisters on hands, feet, knees, elbows |
| Typical cause | Coxsackievirus A, occasionally enterovirus 71 | Coxsackievirus A16 and enterovirus 71 most often3 |
| Age group | Mostly children under 10 | Mostly children under 5 |
| Course | 7 to 10 days, supportive care | 7 to 10 days, supportive care |
If your child only has sores in the back of the mouth with no rash on the body, it’s more likely herpangina. If there’s also a rash on the hands, feet, or buttocks, it’s more likely HFMD. A pediatrician can tell the two apart on exam. The treatment is the same either way: rest, fluids, and pain relief.2
How to Care for Your Child at Home
Herpangina has no specific treatment. Antibiotics and antiviral drugs do not work against enteroviruses.12 Care focuses on keeping your child hydrated, comfortable, and rested while the infection runs its course.
What helps:
- Cold fluids and soft foods — Popsicles, ice cream, smoothies, applesauce, yogurt, and cold milk soothe sore throats. Encourage small sips often, even if appetite is low10
- Pain and fever relief — Ask your pediatrician about acetaminophen or ibuprofen dosing for your child’s age and weight. Do not give ibuprofen to infants under 6 months without medical guidance, and never give aspirin to children
- Saltwater rinses — For older children who can rinse and spit, a warm saltwater rinse a few times a day eases mouth pain10
- Rest in a quiet, well-ventilated room — Helps recovery and limits spread to other family members
- Avoid irritants — Skip hot drinks, citrus juices, spicy foods, salty snacks, and crunchy or acidic foods that sting the sores
Watch hydration closely. Pediatric oral rehydration solutions (like Pedialyte) help if your child won’t drink much water or milk.
What to Eat and Avoid
Many children struggle to swallow when herpangina sores are at their worst, and they refuse to eat. Prioritize fluids over solids. If your child won’t touch food, that’s okay for a few days — staying hydrated is what matters.
Good choices: popsicles, ice cream, cold yogurt, soft bread, scrambled eggs, cold pasta, applesauce.
Avoid: orange juice and citrus drinks, hot soups or tea, spicy foods, salty chips or crackers, carbonated drinks.
Recovery and Immunity
Most children recover fully within 7 to 10 days.4 Recovery usually gives immunity to that specific virus strain, but a child can get herpangina again from a different enterovirus.2
When to Call the Doctor
Call your pediatrician or seek emergency care if your child has any of these red flags. Most herpangina is mild, but these signs need a same-day call or an ER visit.
Call your pediatrician right away if your child:
- Refuses fluids or has not had a wet diaper for 8 hours7
- Shows signs of dehydration: no tears when crying, dry mouth or tongue, sunken eyes, fewer wet diapers, unusual drowsiness7
- Has a rectal temperature of 100.4°F (38°C) or higher and is younger than 3 months old6
- Has a fever over 104°F at any age6
- Has a fever lasting more than 3 days, or a fever that returns after going away6
- Has symptoms lasting more than 7 days
- Has a weakened immune system (cancer treatment, transplant, immune disorder)
- Is a newborn (under 1 month) with any symptoms
Seek emergency care if your child has:
- A stiff neck or persistent severe headache6
- Confusion, extreme drowsiness, or unusual irritability6
- Trouble breathing6
- A seizure
- Persistent vomiting6
If you are pregnant and develop symptoms of herpangina or believe you were exposed, contact your OB-GYN promptly.
A Note on Febrile Seizures
High fevers in young children can occasionally trigger a brief febrile seizure. It is frightening to witness, but most febrile seizures are short and not dangerous on their own.8 If your child has a seizure, lay them on their side on a safe surface, stay with them, do not put anything in their mouth, and call your pediatrician once it passes.8
Call 911 if:8
- It’s your child’s first seizure
- The seizure lasts more than 5 minutes
- Your child has trouble breathing
- Your child was injured during the seizure
- Your child does not wake up afterward
- Another seizure starts before your child has returned to normal
Herpangina in Adults
Adults can get herpangina, though it is less common than in children. Cases have been reported in adolescents and young adults — particularly in parents, caregivers, and teachers exposed to young children — and severity can be higher in adults with weakened immune systems, pregnant people, and newborns exposed to the virus.1
Symptoms in Adults
The symptoms are the same as in children but can feel more intense. Adults more often experience headache, back pain, and body aches alongside the sore throat and mouth sores.1 The illness still typically resolves in 7 to 10 days.
Higher-Risk Adults
Most adults recover without problems. Three groups need closer attention:
- Pregnant people — See the pregnancy section below
- People with weakened immune systems — Cancer treatment, organ transplant, HIV, or immune-suppressing medications can lead to more severe or prolonged illness. Contact your doctor early9
- Newborns under 1 month with symptoms or a known close exposure — Call the pediatrician promptly. Seek immediate medical evaluation if the newborn has a fever, is feeding poorly, seems unusually sleepy, has trouble breathing, or shows any other signs of illness9
Herpangina and Pregnancy
Contact your OB-GYN if you develop herpangina symptoms during pregnancy or are exposed to someone who has it. One older population-based study reported an association between herpangina in pregnancy and outcomes including low birth weight, preterm delivery, and small-for-gestational-age infants.11 The CDC currently states there is no clear evidence that non-polio enterovirus infection during pregnancy increases the risk of miscarriage, stillbirth, or congenital problems, but recommends pregnant people contact their doctor if exposed.9
There is no antiviral treatment for herpangina, so management in pregnancy is supportive: rest, fluids, pain relief approved by your OB, and monitoring for complications.
Treatment for Adults
Adult treatment mirrors pediatric care: rest, fluids, soft cold foods, saltwater rinses, and over-the-counter pain relievers. See your doctor if you have a high fever lasting more than 3 days, severe difficulty swallowing, signs of dehydration, neurological symptoms, or symptoms that last more than 7 days.
How Herpangina Is Diagnosed
A pediatrician or doctor diagnoses herpangina with a physical exam and a review of symptoms. Tests are rarely needed because the sore location — back of the mouth, soft palate, and tonsils — is distinctive.24 In rare cases where a specific enterovirus is suspected — such as severe illness, neurological symptoms, or a local outbreak — a doctor may order a PCR test on a throat or sore swab, a stool sample, or another specimen to identify the virus.4
How to Prevent the Spread of Herpangina
Good hygiene is the strongest protection against herpangina. Research on enterovirus 71 outbreaks found that handwashing by children and adult caregivers significantly reduced transmission.1213
What helps:
- Wash hands often — Use soap and warm water for at least 20 seconds, especially after diaper changes, coughing or sneezing, and before eating. Help young children wash thoroughly
- Disinfect surfaces and toys — Enteroviruses survive on surfaces for hours to days, so wipe down high-touch items (doorknobs, toys, light switches) with an EPA-approved disinfectant9
- Cover coughs and sneezes — Use a tissue or elbow, then wash hands
- Keep sick children home — Keep your child home while they have fever, feel too sick to participate, or have uncontrolled drooling from mouth sores. Follow your daycare, school, and local health department’s return-to-care rules3
- Avoid sharing utensils, cups, or food — Especially within a household when someone is sick
Even after symptoms clear, the virus can shed for weeks in stool. Continue strict handwashing for at least 2 weeks after recovery.1
When to See a Doctor
Herpangina is usually a mild illness that resolves in 7 to 10 days with home care. Call your pediatrician if your child shows signs of dehydration, has a high fever lasting more than 3 days, or has symptoms that persist beyond a week. Seek emergency care for a stiff neck, seizure, trouble breathing, persistent vomiting, or any symptoms in a newborn.
If you’re still unsure what’s causing your child’s mouth sores, our toddler mouth sores guide walks through the most common causes and how to tell them apart.
What Causes Herpangina and How is it Treated?
NewMouth PodcastSources
- Corsino, CB., et al. "Herpangina." StatPearls, 2023.
- Tesini, BL. "Herpangina." Merck Manual Professional Edition, 2024.
- Centers for Disease Control and Prevention. "HFMD: Causes and How It Spreads." CDC, 2024.
- Schwartz, CI. "Herpangina." MedlinePlus Medical Encyclopedia, 2025.
- Klatte, JM. "Coxsackievirus Infections in Children." HealthyChildren.org, American Academy of Pediatrics, 2021.
- American Academy of Pediatrics. "Fever: When to Call the Pediatrician." HealthyChildren.org, 2022.
- American Academy of Pediatrics. "Signs of Dehydration in Infants and Children." HealthyChildren.org, 2019.
- American Academy of Pediatrics. "Febrile Seizures in Children." HealthyChildren.org, 2025.
- Centers for Disease Control and Prevention. "About Non-Polio Enteroviruses." CDC, 2024.
- Stanford Medicine Children's Health. "Herpangina in Children." Stanford Medicine Children's Health, accessed 2026.
- Chen, YH., et al. "Increased risk of adverse pregnancy outcomes among women affected by herpangina." American Journal of Obstetrics and Gynecology, 2010.
- Ruan, F., et al. "Risk Factors for Hand, Foot, and Mouth Disease and Herpangina and the Preventive Effect of Hand-washing." Pediatrics, 2011.
- Liu, J., et al. "Caregivers: the potential infection resources for the sustaining epidemic of hand, foot, and mouth disease/herpangina in Guangdong, China?" Archives of Public Health, 2021.

Experienced medical writer with background in biopsychology and public health.
Related Articles

Are Tonsil Stones Contagious?
Are Tonsil Stones Contagious? No, tonsil stones are not contagious, nor are they serious health problems. While tonsil s...

Can Cavities Go Away on Their Own?
A cavity that has formed a hole in your tooth won't go away. Once a cavity wears through your tooth's enamel, you must s...

Cobblestone Throat: Causes, Symptoms, and Treatment
Cobblestone throat causes raised, bumpy tissue on the back of the throat, usually from postnasal drip, infection, allerg...

Dental Fluorosis: Causes, Symptoms & Treatment
This article offers you a complete guide to dental fluorosis. Read on to learn more about this condition, its causes, pr...