Cleft Lip and Palate: Types, Causes, Risks & Treatment
Reader-supported. We may earn a commission from links on this page. Advertising disclosure.
In this article
What is Cleft Lip and Palate?
Oral clefts appear as splits or openings in the upper lip, palate (roof of the mouth), or both. The splits cause gaps and defects in the affected areas. They are also usually associated with a nose deformity on the same side.
Orofacial clefts, specifically a cleft lip or palate, are among the most common head and neck birth defects. Clefts affect roughly 1 in 700 children worldwide.
In the U.S., cleft lip/palates are most common in Native Americans, Asians, and Latinos. African Americans have the lowest risk of developing orofacial clefts.
Cleft Lip or Palate Health Problems
Cleft palate children may have speech and language problems. However, it can also lead to serious medical and dental issues.
These conditions include:
- Dental problems, such as missing or misaligned teeth
- Greater risk for cavities due to weaker enamel and thicker saliva production
- Hearing problems
- Ear infections
- Feeding problems
- Abnormalities affecting the middle ear
- Psychosocial issues
Half of all clefts involve both the lip and palate. A cleft that only affects the palate is a less common birth defect.
Other Side Effects of a Cleft Lip and Palate
Common medical conditions associated with cleft lip and palate include:
- Van der Woude syndrome – Affects facial development
- CHARGE syndrome – Causes coloboma, heart defects, atresia choanae, and ear abnormalities
- Apert syndrome – Causes abnormal skull growth and affects the shape of the face and head
- Pierre Robin sequence – A birth defect that results in a smaller jaw, breathing difficulties, and a tongue that falls back in the throat
- Kabuki syndrome – A congenital disorder that causes abnormal facial features
- Klippel Feil syndrome – Causes neck and spine abnormalities and results in a shorter neck
- Stickler syndrome – Causes eye abnormalities, hearing loss, joint problems, and a flattened facial appearance
- Treacher-Collins syndrome – Causes ears, eyes, cheekbones, and chin deformities
- DiGeorge syndrome – A chromosomal disorder that can cause poor heart development, issues with the immune system, and a cleft palate
- Beckwith-Wiedemann syndrome – Children with this syndrome have an abnormally large tongue, resulting in breathing, swallowing, and speaking difficulties
- Goldenhar syndrome – A birth defect that causes poor development of the nose, soft palate, lips, mouth, and ears
Types of Cleft Lip
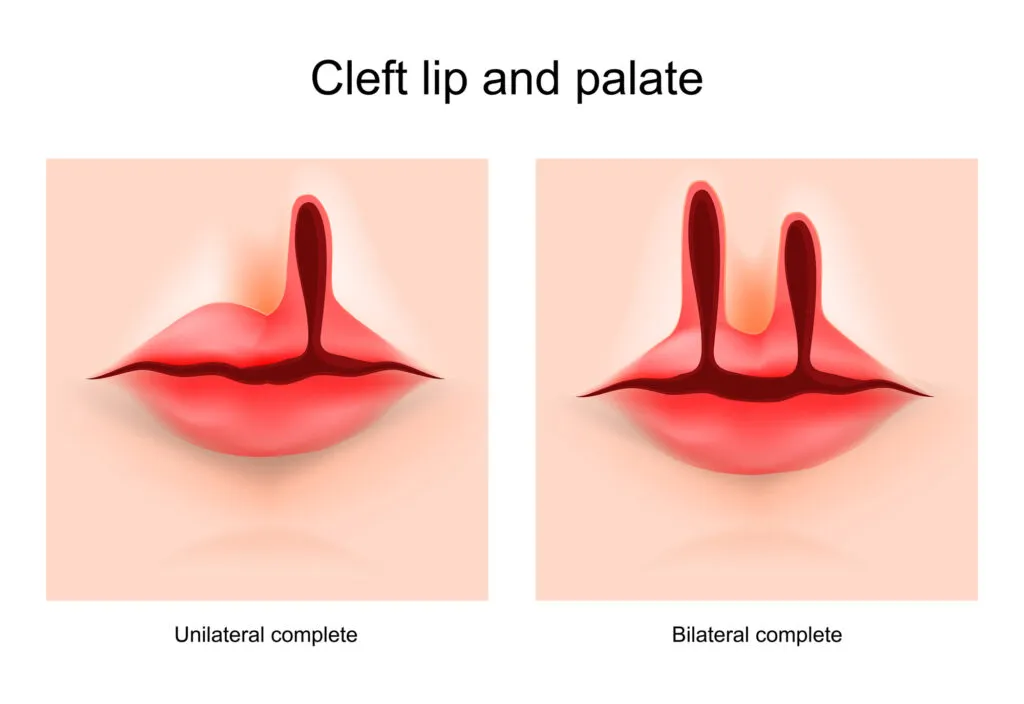
Cleft lips can either be complete or incomplete, which means the splits may or may not extend to the nose. They can also develop on one side (unilateral) or both sides (bilateral) of the upper lip.
There are a few types of cleft lips:
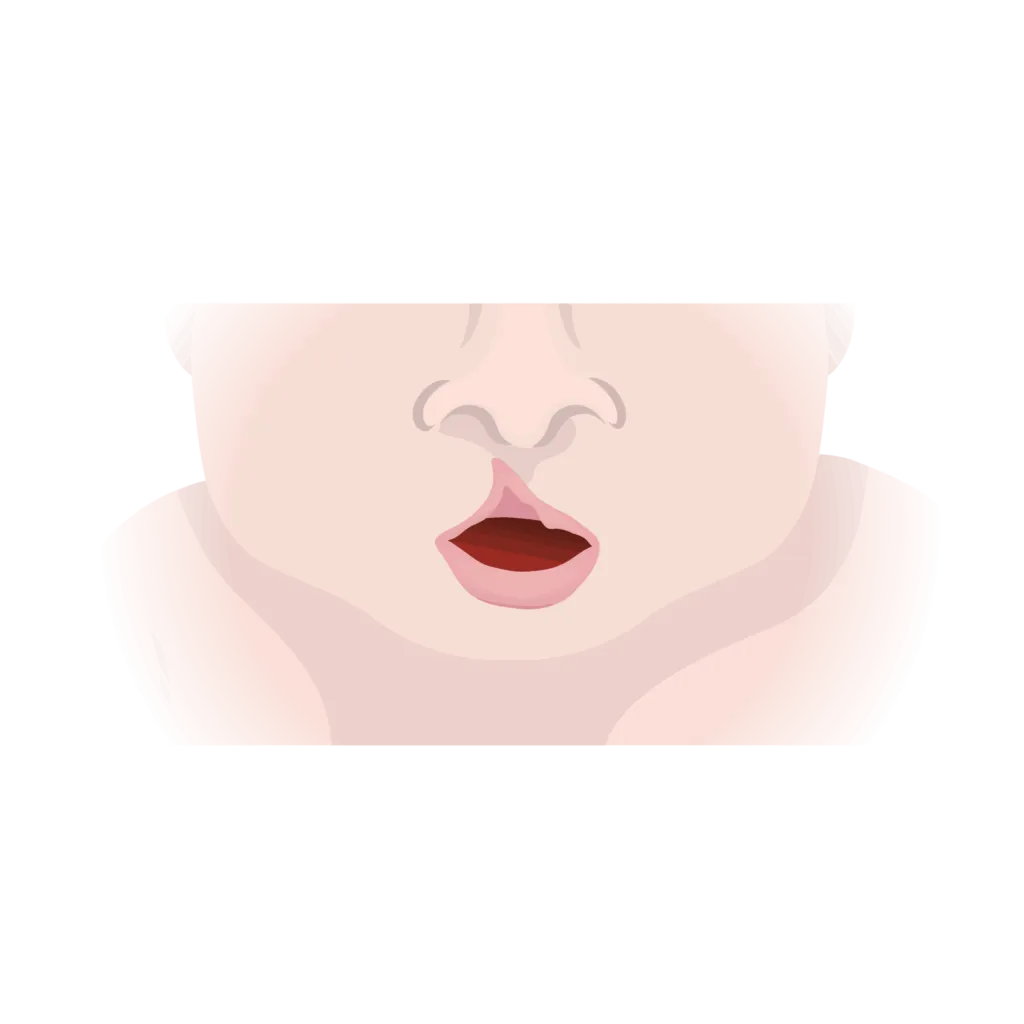
Incomplete Unilateral
Clefts that develop on one side of the upper lip and do not extend into the nose.
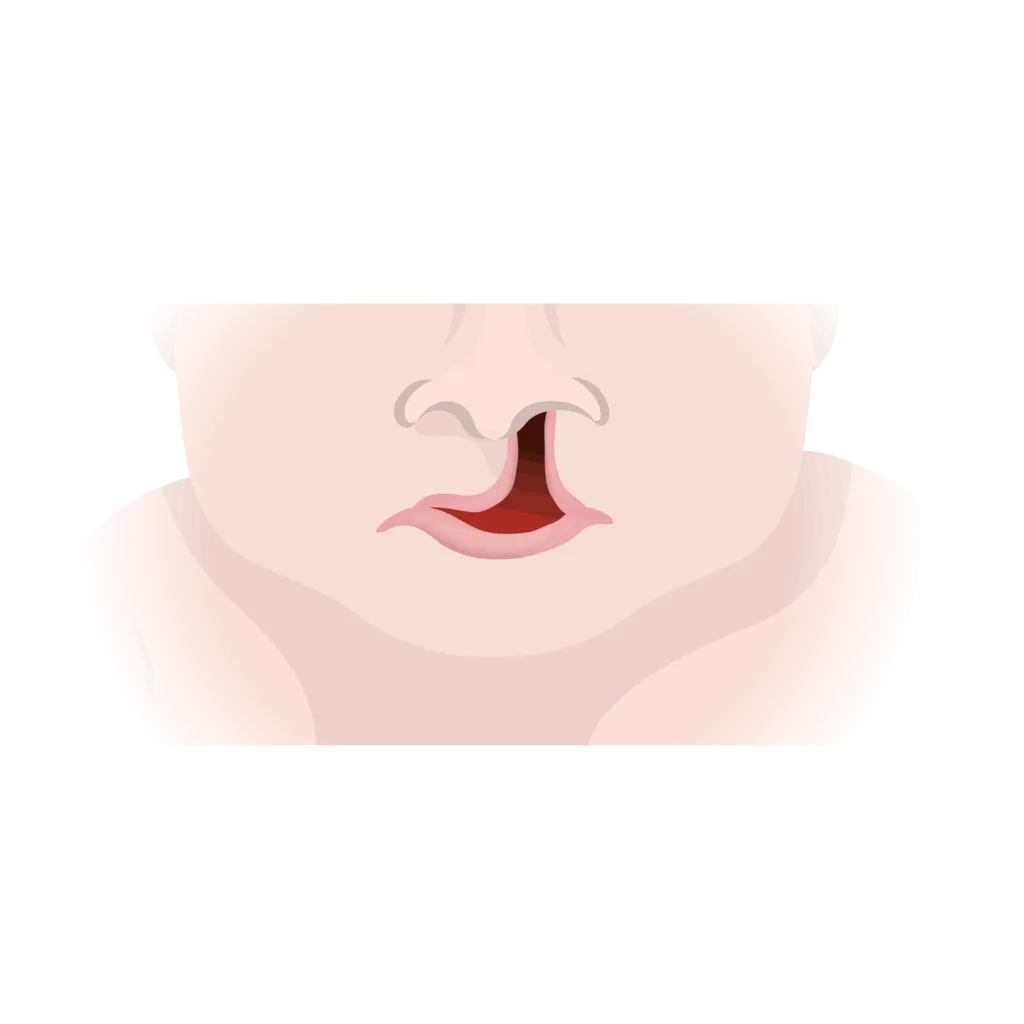
Complete Unilateral
Clefts that develop on one side of the upper lip and extend into the nose.
Incomplete Bilateral
Clefts that appear on both sides of the upper lip but do not extend into the nose.
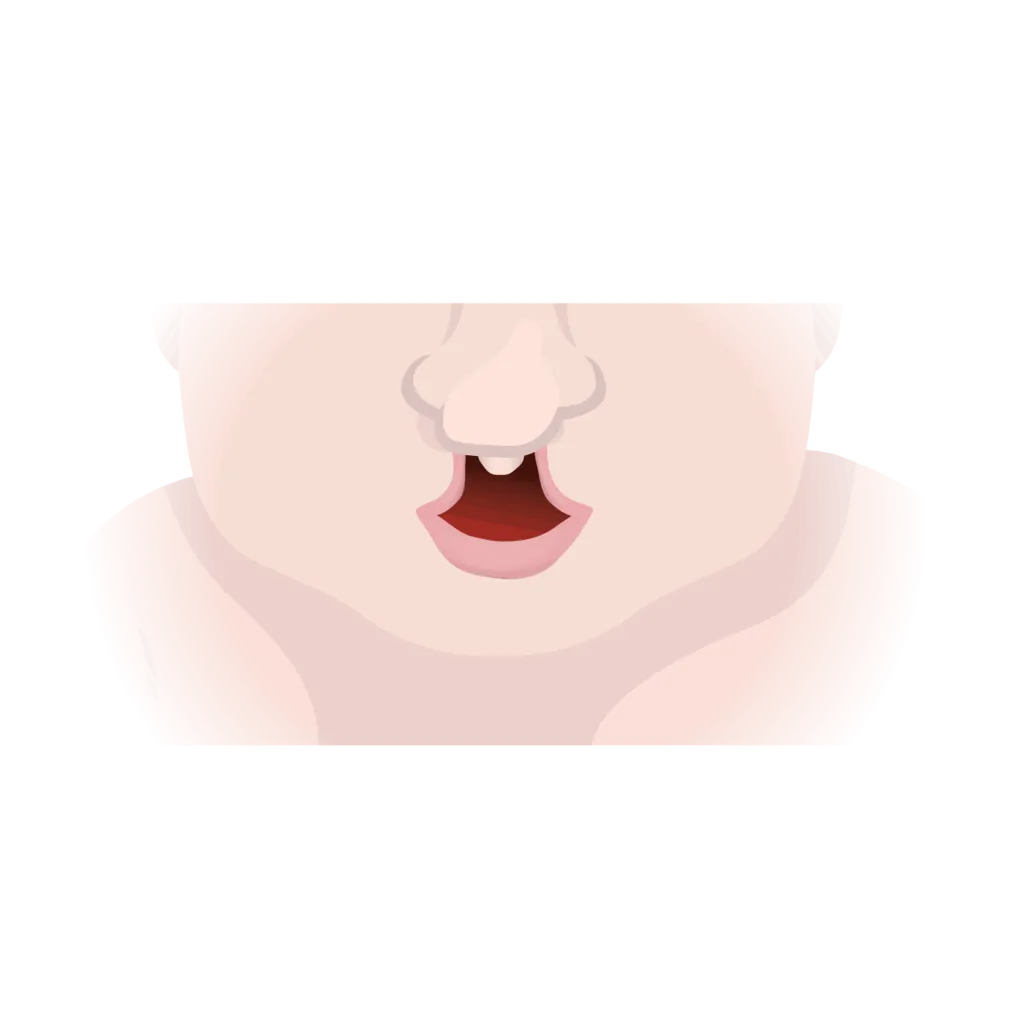
Complete Bilateral
Clefts that appear on both sides of the upper lip and extend into the nose.
Types of Cleft Palate
Like cleft lips, cleft palates can be complete or incomplete, meaning the splits may involve the primary (front) palate, secondary (back) palate, or both.
There are a few types of cleft palates:
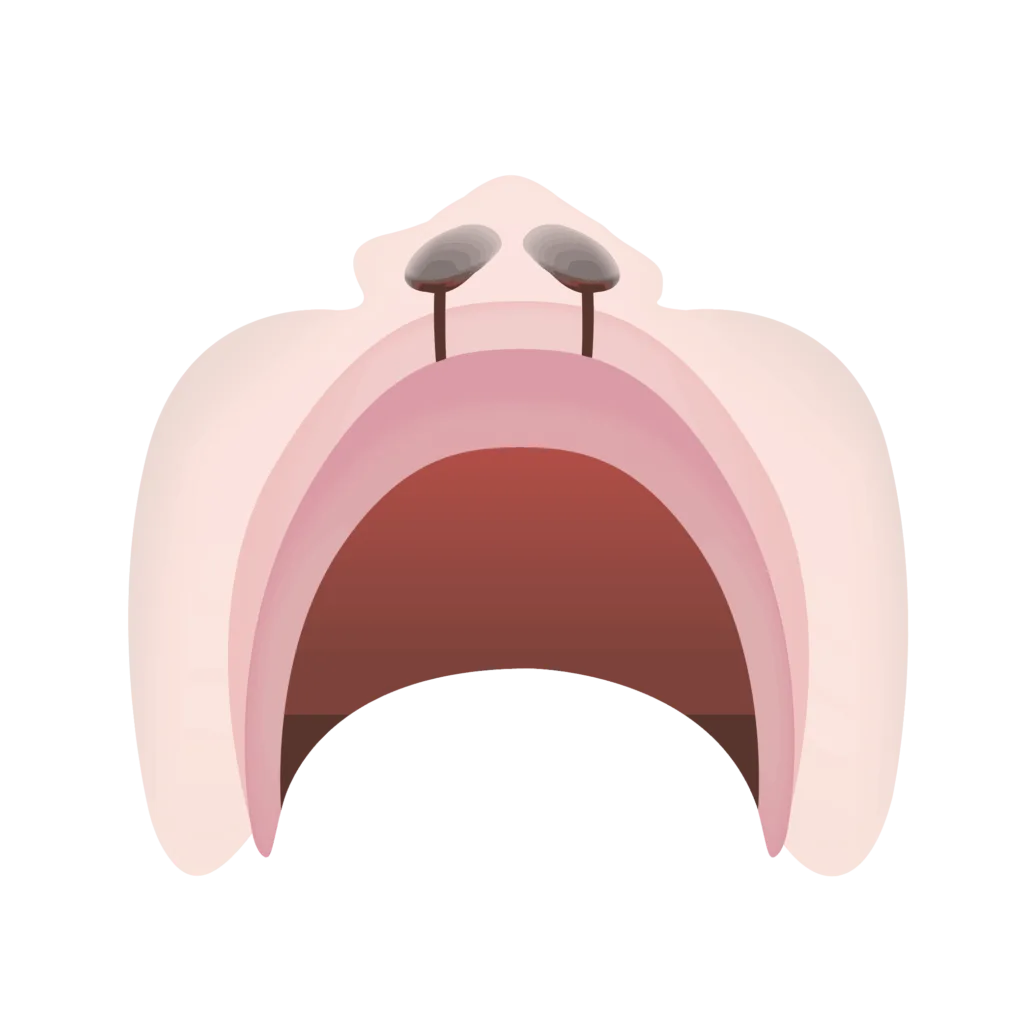
Incomplete Cleft Palate
Clefts that develop in the soft palate (back of the mouth).
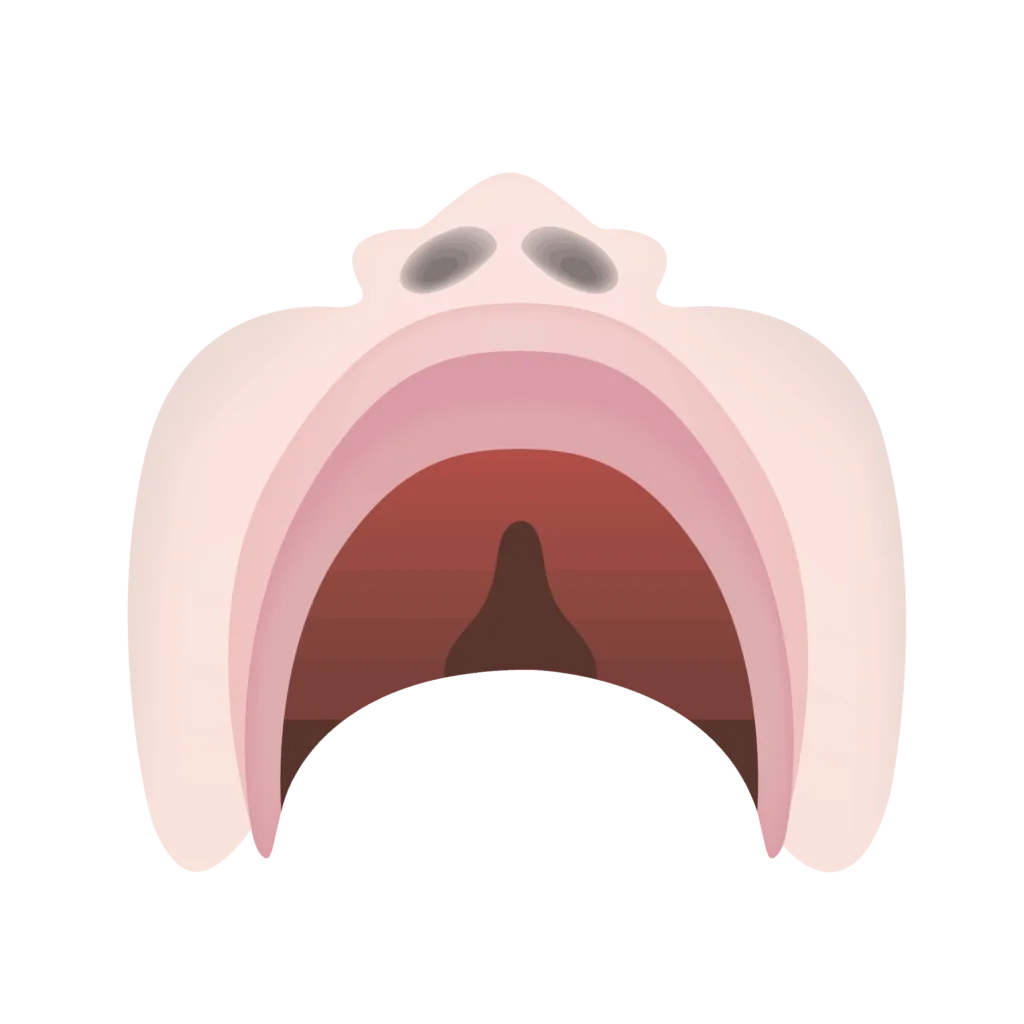
Complete Cleft Palate
Clefts that develop in the soft and hard palate on one side of the mouth. The splits extend past the lips and into the nose.
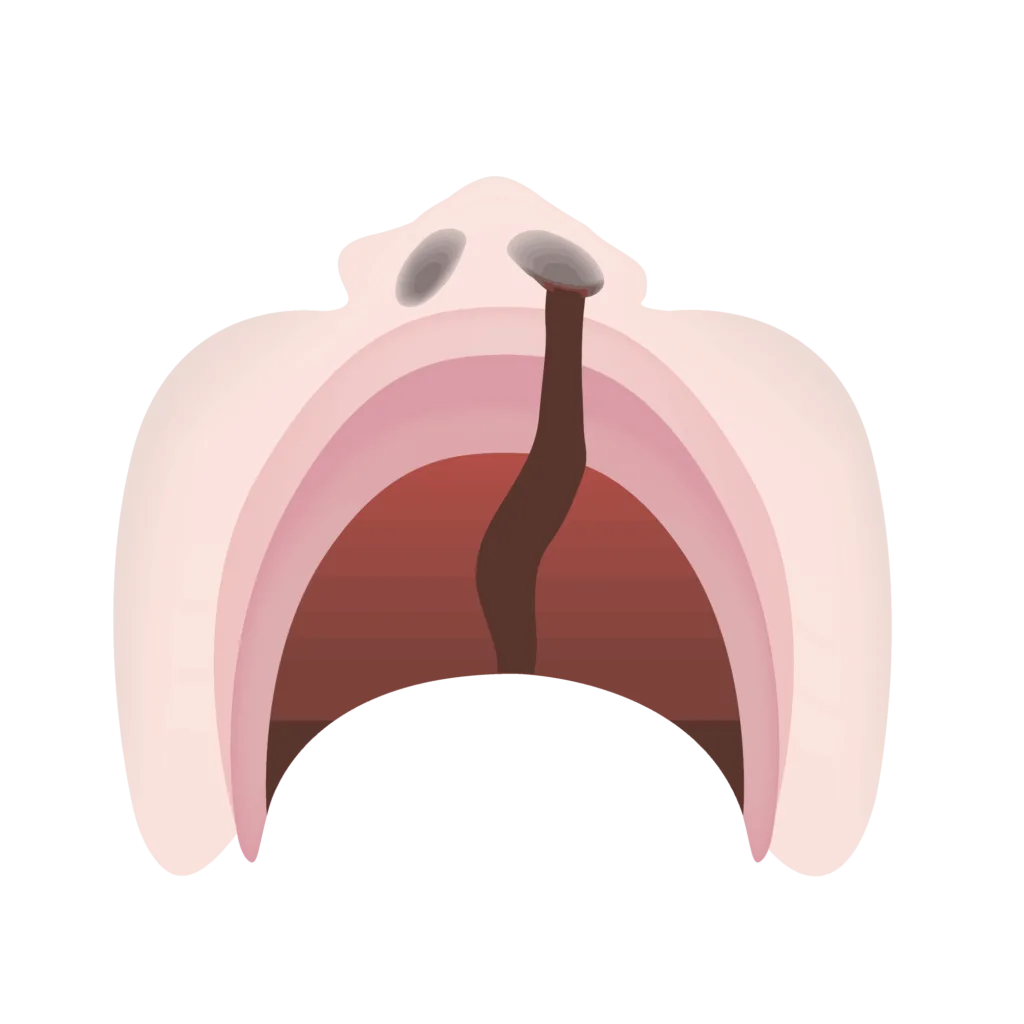
Unilateral Complete Cleft Palate and Lip
Clefts that develop in the soft and hard palate on one side of the mouth. The splits extend past the lips and into the nose.
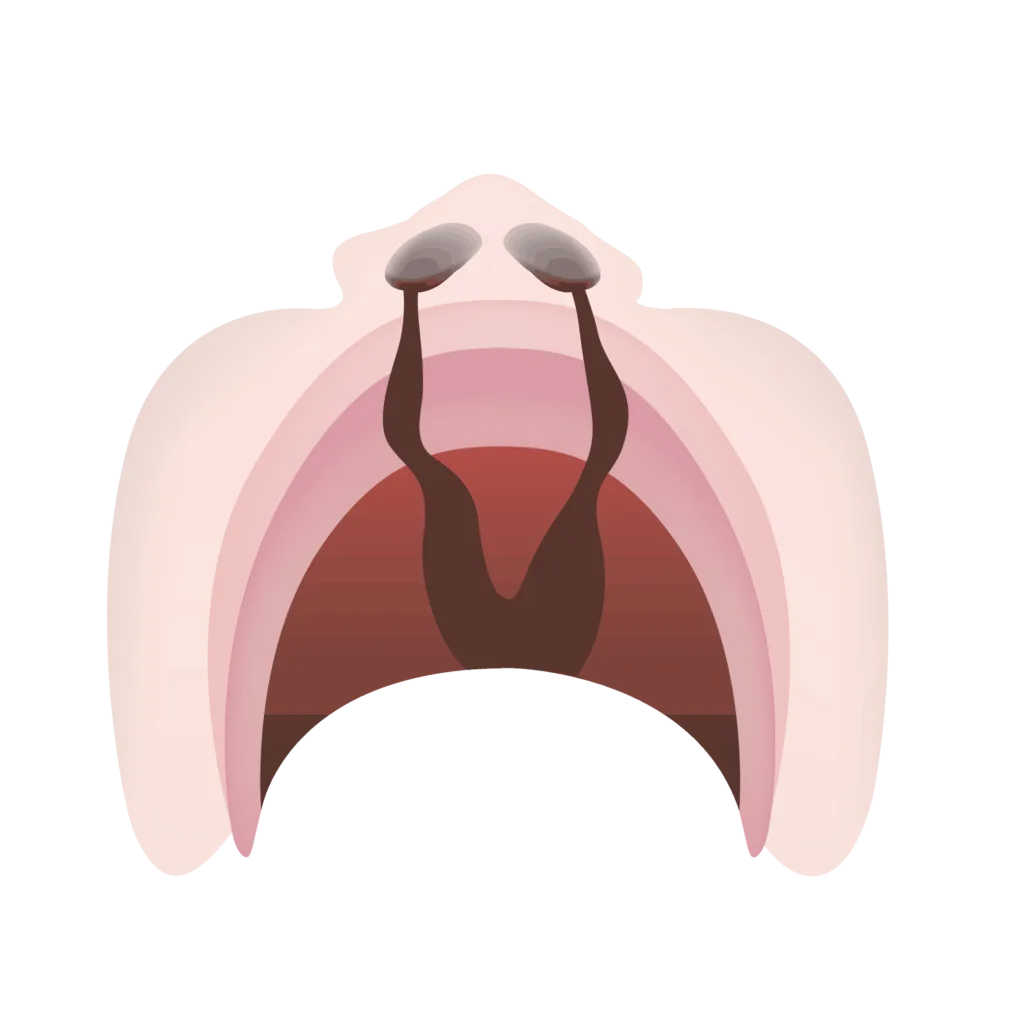
Complete Bilateral Cleft Lip and Palate
Clefts that develop in the soft and hard palate on both sides of the mouth. The splits extend past the lips and into the nose.
Submucous Cleft Palate
A submucous cleft palate affects the palate and uvula, the teardrop-shaped tissue hanging in the back of your throat. The soft palate and uvula work together to prevent food from going up your nose.
Someone with a submucous cleft palate has a cleft underneath the mucous membrane. This type of cleft is “hidden” and will not be noticeable until the baby is born. It develops in about 1 in 1,200 babies.
Isolated Cleft Palate
A term used when a cleft occurs in the palate only, with no cleft lip present. One in 2,000 babies are born with this type of cleft. It’s also typically difficult to see.
What Causes Cleft Palate?
Clefts are birth defects caused by genetic and environmental factors. Common reasons a child may develop a cleft lip and/or palate include:
- Family history of cleft lip and palate
- Having diabetes during pregnancy is linked to birth defects, such as cleft lips
- Obesity during pregnancy can increase the risk of cleft lip and palate
- Exposure to unhealthy substances during pregnancy, such as cigarettes, alcohol, and some medications
- Exposure to Rubella or other infections
Medications That May Cause a Cleft Palate
Some medications can affect your baby during pregnancy and increase the likelihood of a cleft lip or palate.
These medications include, but are not limited to:
- Accutane
- Methotrexate
- Seizure medications
- Anticonvulsant medications
How is a Cleft Palate Diagnosed?
A prenatal ultrasound can detect a cleft lip or palate after 16 weeks of pregnancy. The diagnosis is confirmed at birth with a physical examination.
An incomplete cleft lip or an isolated palate may not be seen on an ultrasound. Because of this, these types of clefts can be diagnosed for the first time at birth.
They’ll also perform a thorough exam to determine if the cleft involves both the soft and hard palate or the soft palate alone. In some cases, a cleft is diagnosed on a fetal MRI.
Phases of Cleft Palate Treatment
Children born with a cleft lip, palate, or both require multiple phases of treatment starting from birth and into early adulthood (18+ years old). Treatment typically includes:
- Adhesions
- Repairs
- Surgeries
- Bone grafts
- Orthodontic treatment
Cleft lip and palate repairs are performed by a plastic surgeon, pediatric otolaryngologist, or an oral and maxillofacial surgeon with extensive training in pediatric craniomaxillofacial surgery. There are a few phases of treatment throughout childhood, depending on the child’s needs.
Birth: Orthopedic Treatment and Lip Repair
Children with cleft lip and palate from birth require pre-surgical infant orthopedics (PSIO). In particular, this procedure reshapes nasal and alveolar segments before cleft lip surgery.
Most babies typically have surgery early in life to repair cleft lip and palate, typically between 3 and 6 months of age. A nasolabial (lip) adhesion may also be necessary before repairing the cleft lip to reduce tension and speed up recovery.
Palate Repair (1 Year)
A cleft palate repair is completed between 9 and 18 months, typically around age 1. Early palate repair allows for better speech development.
Repairing the defect early creates more scar tissue and may lead to improper mouth growth, improper bite, and poor facial esthetics. Orthodontic treatment is typically necessary later on to correct these issues. If palate repair is completed after 18 months, speech can be negatively impacted.
Velopharyngeal Surgery (2-3 Years)
Velopharyngeal insufficiency (VPI) occurs when the soft palate does not close tightly against the back of the mouth. This typically leads to abnormal speech and/or hypernasality. Velopharyngeal surgery is completed around 3 years of age if a child’s speech does not improve.
Alveolar Bone Grafts and Maxillary Expansion (5-9 Years)
After a cleft lip and palate repair, a surgeon performs alveolar bone graft surgery a few years later. The surgery adds bone to the gum ridge in children born with clefts. In addition, the bone graft must be completed as a child begins to lose their baby teeth before permanent teeth grow.
Phase I Orthodontic Treatment (11 Years)
As baby teeth fall out and permanent teeth grow in (the mixed dentition phase), the first round of orthodontic treatment occurs. Orthodontic treatment typically:
- Aligns the roof of the mouth
- Fixes crossbites
- Creates space for erupting permanent teeth
- Treats impacted teeth
Phase II Orthodontic Treatment (13-15 Years)
By age 13, all permanent teeth have erupted. An additional phase of orthodontic treatment may also be necessary to align teeth and fix any dental abnormalities.
Orthognathic Surgery and Final Restorative Care (18+ Years)
Orthognathic surgery is an operation that corrects the alignment of the jaws. It may be necessary after the cleft lip repair, bone graft surgery, and orthodontic treatment.
How Do You Prevent Cleft Palate in Babies?
Ways to help prevent cleft lip during pregnancy include:
- Eat a balanced diet
- Do not drink alcohol
- Take folic acid supplements (600 micrograms per day)
- Do not smoke cigarettes, recreational drugs, or other tobacco products
- Make sure the medications you are taking during pregnancy are safe
- Make sure you are free from infections
- Gain a healthy amount of weight
- Get prenatal care during pregnancy
Sources
- Ahlin, J.H. “Maxillofacial Orthopedics: A Clinical Approach for the Growing Child.” Quintessence Publ., 2003.
- Angulo-Castro et al. “Maternal Risk Factors Associated with the Development of Cleft Lip and Cleft Palate in Mexico: A Case-Control Study.” Iran J Otorhinolaryngol, 2017.
- “Cleft Lip and Palate.” CHLA, 2019.
- “Development of Cleft Lip & Palate.” University of Virginia, 2019.
- Nowak, A. “Pediatric Dentistry: Infancy through Adolescence.” Elsevier, 2019.
- Sreejith et al. “Psychological Effect of Prenatal Diagnosis of Cleft Lip and Palate: A Systematic Review.” Contemp Clin Dent, 2018.

Experienced general dentist and adjunct professor. Advocates for preventive dentistry and dental education.

Lead content writer and certified nutritionist focusing on clear aligners and teeth whitening.
Related Articles

Fluoride Treatment: Uses, Benefits & Risks
What is fluoride? Learn about fluoride treatment in the United States, including its benefits, risks, and how it helps p...

Baby Tooth Extractions: Causes, Procedure Steps & Aftercare
Are baby tooth extractions necessary? Here are five reasons to consider the procedure for your child, including tips to...
Stainless Steel Crowns: What They Are and How They Work
Stainless steel crowns are dental restorations that cover a tooth's entire chewing surface. Read on for stainless steel...

What Is Bottle Rot and How Do You Prevent It?
Bottle rot is a common condition that can affect babies and children. Learn how to prevent it, what symptoms to look for...